
Clinical Profile and Surgical Outcomes of Pediatric Umbilical Pilonidal Sinus

Abstract
Introduction
Umbilical pilonidal sinus (UPS) is a rare form of pilonidal disease (PNS) predominantly affecting young individuals. Owing to its low incidence, data on risk factors and optimal management remain limited. This study aimed to investigate UPS in the pediatric age group and evaluate the efficacy of surgical management.
Methods
A retrospective, single-center cohort study was conducted over five years, including patients aged ≤18 years diagnosed with UPS. Clinical, demographic, and risk factor data were collected from medical records. All patients underwent surgical management under local anesthesia, with follow-up to assess healing and recurrence. Descriptive statistical analysis was performed using SPSS version 27.0.
Results
A total of 42 cases (mean age 16.4 ± 1.48 years) were included. Males comprised 22 (52.4%) of cases. Dense body hair was observed in 29 (69.0%) of patients, and 15 (35.7%) reported a positive family history, and obesity was common (median body mass index (BMI) was 25.9 (IQR: 22.5–29.0)). Surgical treatment achieved successful healing in 40 (95.2%) of cases, with a low recurrence rate of 1 (2.4%).
Conclusion
Surgical management showed favorable outcomes with high healing and low recurrence rates, supporting its effectiveness in pediatric patients. However, larger multicenter studies are needed to clarify risk factors and optimize management strategies.
Introduction
Pilonidal sinus (PNS) disease is the formation of a sinus tract containing hair and debris, most frequently occurring in the sacrococcygeal region [1]. The condition typically results from friction and the insertion of loose hairs into the skin, provoking a chronic inflammatory and foreign-body response. While the sacrococcygeal area is the classic site, PNS has also been reported in other locations, including the axilla, groin, inter-digital spaces, and the umbilicus [2,3].
Umbilical pilonidal sinus (UPS) is a rare clinical entity, with an estimated incidence of approximately 0.6% of all PNS cases. The pathogenesis is thought to be similar to that of sacrococcygeal PNS [2,4].
Umbilical pilonidal sinus is primarily seen in young, post-pubertal individuals. Approximately 85% of patients are younger than 30 years, a distribution attributed to the onset and peak of body hair growth following puberty [2]. Because umbilical PNS is rare, its clinical features and risk factors are poorly defined; its origin remains controversial, with no clear consensus on pathophysiology or optimal management [4,5].
Therefore, the current study aims to investigate UPS in the pediatric age group and evaluate the efficacy of surgical management. All references cited herein were thoroughly reviewed to avoid inclusion of non-peer-reviewed data [6].
Methods
Study design
This single-center, retrospective cohort study was conducted at a private medical facility over a period of five years. It included pediatric patients with UPS who underwent evaluation, treatment, and follow-up at the same center.
Setting and participants
This study included patients diagnosed with UPS who presented to the clinic during the study period. Clinical and sociodemographic data were obtained from patient records and the attending healthcare providers. The recorded variables comprised age, gender, body mass index (BMI), family history of PNS, presence of other types of PNS, presenting symptoms, clinical examination findings, postoperative complications, and follow-up.
Inclusion and exclusion criteria
Patients eligible for this study were those aged 18 years or younger with a diagnosis of UPS. These included patients presenting with typical symptoms of UPS, such as umbilical discharge (serous, purulent, or bloody), pain, swelling, or a visible tuft of hair within the umbilicus, who received treatment at the clinic during the study period and completed follow-up. Patients older than 18 years, those with alternative causes of umbilical infection or discharge, or those with incomplete medical records were excluded.
Surgical management
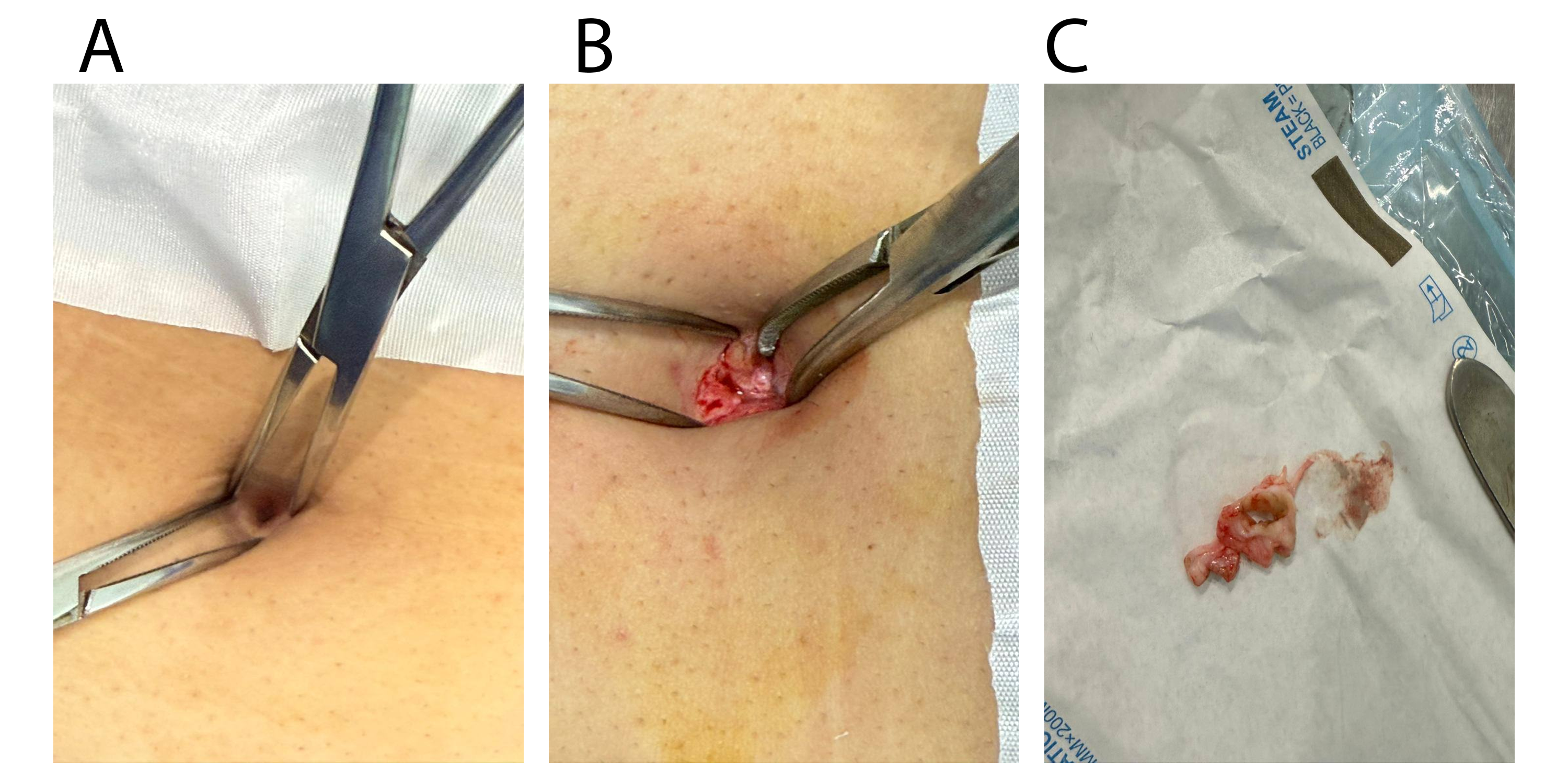
All pediatric patients underwent a comprehensive preoperative assessment to determine their suitability for surgery under local anesthesia. The preoperative evaluation included monitoring of vital signs, viral screening, and hematological assessment. All surgical procedures were performed under local anesthesia with the patient in the supine position using strict aseptic technique. In patients with non-acutely infected UPS disease or those presenting with minimal infection, the surgical procedure consisted of excision of the pilonidal sinus and its tracts through a minimal incision within the umbilicus. The wound was then left open to heal by secondary intention. For patients presenting with an acutely infected umbilical pilonidal abscess, management was performed in two stages. The first stage involved incision and drainage of the abscess followed by daily wound dressing with gauze drainage. Definitive excision of the sinus tract was performed in a second stage after resolution of the acute infection (Figure 1).
Statistical analysis
The data were organized and analyzed using Microsoft Excel 2019. Descriptive analysis was conducted using the Statistical Package for Social Sciences (SPSS) version 27.0. The statistical tests used included the Shapiro-Wilk test for normality, and because the data were not normally distributed and the sample size was small, the Mann Whitney U test was used. Categorical variables were analyzed using Fisher’s exact test when the expected cell frequencies were less than 5 in more than 20% of the cells, and a p-value < 0.05 was considered statistically significant. The results are presented as frequencies, percentages, means, ranges, medians, interquartile ranges (IQR) and exact p values.
Results
The study included 42 cases, including one recurrence identified after 2 years. The patients were aged between 13 and 18 years, with a mean age of 16.4 ± 1.48 years. Slight male predominance was observed, accounting for 22 (52.4%) of the cases. Most participants were students, accounting for 37 (88.1%) patients. Regarding body mass index (BMI), the median BMI was 25.9 (IQR: 22.5–29.0); 17 (40.5%) patients had a healthy BMI, while 14 (33.3%) were overweight and 11 (26.2%) were obese. None of the patients had a previous medical history, whereas 5 (11.9%) had a previous surgical history. In addition, a positive family history was reported in 15 (35.7%) of the cases (Table 1).
|
Variable |
Frequency/Percentage (%) |
|
Age |
13-18 (16.4 ± 1.48) |
|
BMI |
|
|
Median (IQR) |
25.9 (22.5-29.0) |
|
Under-weight |
0 (0.0%) |
|
Healthy |
17 (40.5%) |
|
Over-weight |
14 (33.3%) |
|
Obese |
11 (26.2%) |
|
Sex |
|
|
Male |
22 (52.4%) |
|
Female |
20 (47.6%) |
|
Occupation |
|
|
Students |
37 (88.1%) |
|
Worker |
4 (9.5%) |
|
Jobless |
1 (2.4%) |
|
PMH |
|
|
Yes |
0 (0%) |
|
No |
42 (100%) |
|
PSH |
|
|
Yes |
5 (11.9%) |
|
No |
37 (88.1%) |
|
FHx |
|
|
Yes |
15 (35.7%) |
|
No |
27 (64.3%) |
| BMI: Body Mass Index, PMH: Past Medical history, PSH: Past surgical history, FHx: Family history | |
Most patients were non-smokers, accounting for 40 (95.2%) cases, while only 1 (2.4%) patient reported active smoking and 1 (2.4%) reported passive smoking exposure. A sedentary lifestyle was observed in 38 (90.5%) patients, whereas only 4 (9.5%) did not report a sedentary lifestyle. Frequent travelling by car was uncommon and was reported in only 1 (2.4%) patient. Body hair was present in all cases (100%). Regarding body hair characteristics, dense or thick body hair was the most common pattern, observed in 29 (69.0%) patients, while 13 (31.0%) had moderate or sparse body hair. In addition, black body hair color was predominant, accounting for 41 (97.6%) cases (Table 2).
|
Variable |
Frequency/Percentage |
|
Smoking |
|
|
No |
40 (95.2 %) |
|
Yes |
1(2.4 %) |
|
Passive |
1(2.4 %) |
|
Sedentary lifestyle |
|
|
Yes |
38 (90.5 %) |
|
No |
4(9.5%) |
|
Frequent travelling by car |
|
|
Yes |
1(2.4%) |
|
No |
41(97.6%) |
|
Body hair presence |
|
|
Yes |
42 (100%) |
|
No |
0 (0.0%) |
|
Type of body hair |
|
|
Dense / Thick |
29 (69.0%) |
|
Moderate/ Sparse |
13 (31.0%) |
|
Body hair Color |
|
|
Yellow |
1(2.4%) |
|
Black |
41(97.6%) |
Regarding the clinical presentation, most patients presented with symptoms lasting for months, accounting for 17 (40.5%) cases, followed by weeks in 13 (31.0%) patients, while 6 (14.3%) presented within days and another 6 (14.3%) after years of symptoms. Nearly all patients were symptomatic, accounting for 41 (97.6%) cases. Discharge was the most common clinical presentation, reported in 35 (83.3%) patients, and purulent discharge was observed in 26 (61.9%) cases. Pain was present in 34 (81.0%) patients, whereas itching and swelling were reported in 17 (40.5%) and 10 (23.8%) patients, respectively. Regarding sinus openings, a single sinus opening was the most frequent finding, observed in 20 (47.6%) patients. Granuloma formation was present in 10 (23.8%) cases, while abscess formation was uncommon and observed in only 3 (7.1%) patients (Table 3). Regarding the significant associations, BMI was significantly associated with itching (p = 0.002) and purulent discharge (p = 0.009). Sex showed a significant association with pain (p = 0.047), while sinus presence was significantly associated with swelling (p = 0.041). In addition, longer UPS duration was significantly associated with itching (p = 0.039) (Table 4).
|
Variables |
Frequency/Percentage |
|
Duration* |
|
|
Days (< 1 week) |
6 (14.3%) |
|
Weeks |
13 (31.0%) |
|
Months |
17 (40.5%) |
|
Years |
6 (14.3%) |
|
Symptomatic |
|
|
Yes |
41(97.6%) |
|
No |
1(2.4%) |
|
Pain |
|
|
Yes |
34 (81.0%) |
|
No |
8 (19.0%) |
|
Swelling |
|
|
Yes |
10 (23.8%) |
|
No |
32 (76.2%) |
|
Itching |
|
|
Yes |
17 (40.5%) |
|
No |
25 (59.5%) |
|
Discharge |
|
|
Yes |
35 (83.3%) |
|
No |
7 (16.7%) |
|
Purulent discharge |
|
|
Yes |
26 (61.9%) |
|
No |
16 (38.1%) |
|
Sinus Number* |
|
|
0 |
11 (26.2%) |
|
1 |
20 (47.6%) |
|
2 |
7 (16.7%) |
|
3 |
1(2.4%) |
|
4 |
1(2.4%) |
|
6 |
2 (4.8%) |
|
Has granuloma |
|
|
Yes |
10 (23.8%) |
|
No |
32 (76.2%) |
|
Abscess formation |
|
|
Yes |
3 (7.1%) |
|
No |
39 (92.9%) |
|
*Percentages may not sum to 100 due to rounding |
|
|
Variables |
Symptoms |
|||||||||
|
Pain |
Swelling |
Itching |
Discharge |
Purulent Discharge |
||||||
|
no |
yes |
no |
yes |
no |
yes |
no |
yes |
no |
yes |
|
|
BMI Healthy Over weight Obese |
5 (11.9%) 1 (2.4%) 2 (4.8%) |
12 (28.6%) 13 (31.0%) 9 (21.4%) |
12 (28.6%) 12 (28.6%) 8 (19.0%) |
5 (11.9%) 2 (4.8%) 3 (7.1%) |
14 (33.3%) 3 (7.1%) 8 (19.0%) |
3 (7.1%) 11 (26.2%) 3 (7.1%) |
1 (2.4%) 4 (9.5%) 2 (4.8%) |
16 (38.1%) 10 (23.8%) 9 (21.4%) |
2 (4.8%) 9 (21.4%) 5 (11.9%) |
15 (35.7%) 5 (11.9%) 6 (14.3%) |
|
p-value |
0.321 |
0.653 |
0.002* |
0.253 |
0.009* |
|||||
|
Sex Female Male |
1 (2.4%) 7 (16.7%) |
19 (45.2%) 15 (35.7%) |
15 (35.7%) 17 (40.5%) |
5 (11.9%) 5 (11.9%) |
10 (23.8%) 15 (35.7%) |
10 (23.8%) 7 (16.7%) |
4 (9.5%) 3 (7.1%) |
16 (38.1%) 19 (45.2%) |
10 (23.8%) 6 (14.3%) |
10 (23.8%) 16 (38.1%) |
|
p-value |
0.047* |
1 |
0.231 |
0.691 |
0.130 |
|||||
|
Sinus Presence No Yes |
1 (2.4%) 7 (16.7%) |
10 (23.8%) 24 (57.1%) |
11 (26.2%) 21 (50.0%) |
0 (0.0%) 10 (23.8%) |
6 (14.3%) 19 (45.2%) |
5 (11.9%) 12 (28.6%) |
1 (2.4%) 6 (14.3%) |
10 (23.8%) 25 (59.5%) |
6 (14.3%) 10 (23.8%) |
5 (11.9%) 21 (50.0%) |
|
p-value |
0.657 |
0.041* |
0.733 |
0.654 |
0.281 |
|||||
|
Granuloma Presence No Yes |
5 (11.9%) 3 (7.1%) |
27 (64.3%) 7 (16.7%) |
24 (57.1%) 8 (19.0%) |
8 (19.0%) 2 (4.8%) |
17 (40.5%) 8 (19.0%) |
15 (35.7%) 2 (4.8%) |
6 (14.3%) 1 (2.4%) |
26 (61.9%) 9 (21.4%) |
11 (26.2%) 5 (11.9%) |
21 (50.0%) 5 (11.9%) |
|
p-value |
0.369 |
1 |
0.162 |
1 |
0.465 |
|||||
|
Abscess Presence No Yes |
8 (19.0%) 0 (0.0%) |
31 (73.8%) 3 (7.1%) |
31 (73.8%) 1 (2.4%) |
8 (19.0%) 2 (4.8%) |
23 (54.8%) 2 (4.8%) |
16 (38.1%) 1 (2.4%) |
7 (16.7%) 0 (0.0%) |
32 (76.2%) 3 (7.1%) |
16 (38.1%) 0 (0.0%) |
23 (54.8%) 3 (7.1%) |
|
p-value |
1 |
0.136 |
1 |
1 |
0.275 |
|||||
|
UPS duration Median (IQR) |
14(3-296.25) |
45 (7-95.5) |
25 (7-90) |
135 (7-547) |
14 (7-75) |
90 (18.5-287) |
7 (5-90) |
60 (7-112) |
7 (5.5-90) |
60 (7-129) |
|
p-value |
0.419 |
0.058 |
0.039* |
0.323 |
0.162 |
|||||
|
Age at presentation Median (IQR) |
16.5 (15.25-17.75) |
17 (16-18) |
17 (16-17) |
17 (14.75-18) |
17 (16-18) |
17 (14.5-17) |
17 (16-17) |
17 (16-18) |
17 (16-17) |
17 (15.75-18) |
|
p-value |
0.792 |
0.682 |
0.384 |
0.876 |
0.372 |
|||||
|
Number of sinuses Mean (Range) |
0.88 (0-1) |
1.35 (0-6) |
1.19 (0-6) |
1.5 (1-4) |
1.2 (0-6) |
1.35 (0-4) |
1.71 (0-6) |
1.17 (0-6) |
1.25 (0-6) |
1.27 (0-6) |
|
p-value |
0.594 |
0.150 |
0.278 |
0.515 |
0.677 |
|||||
|
Total |
8 (19.0%) |
34 (81.0%) |
32 (76.2%) |
10 (23.8%) |
25 (59.5%) |
17 (40.5%) |
7 (16.7%) |
35 (83.3%) |
16 (38.1%) |
26 (61.9%) |
| UPS = umbilical pilonidal sinus; IQR = interquartile range; BMI = body mass index; * indicates statistically significant association (p < 0.05). | ||||||||||
Regarding treatment outcomes, abscess drainage was required in only 2 (4.8%) patients, while the majority of cases did not require drainage. Successful healing was achieved in 40 (95.2%) patients, whereas only 2 (4.8%) did not achieve complete healing. Recurrence was uncommon and was observed in only 1 (2.4%) patient during follow-up (Table 5).
|
Variables |
Frequency/Percentage |
|
Abscess drainage required |
|
|
Yes |
2 (4.8%) |
|
No |
40(95.2%) |
|
Healing |
|
|
Yes |
40(95.2%) |
|
No |
2 (4.8%) |
|
Recurrence |
|
|
Yes |
1(2.4%) |
|
No |
41(97.6%) |
Discussion
There have been conflicting reports in the literature regarding the pathogenesis of UPS, although the exact etiology of UPS remains unclear, some experts suggest that it is an acquired disease. Predisposing factors for UPS disease, include young age, male gender, excessive hairiness, a deep umbilicus and poor personal hygiene [1,7]. There have been reports of cases suggesting an association between PNS disease and other related conditions, including the presence of sinuses at multiple anatomical sites. Such findings support the concept of an acquired etiology, driven by common predisposing factors rather than a congenital origin. This perspective can be extended to UPS, where similar mechanisms and risk factors are likely involved in its development [8–10].
Pilonidal sinus disease is a disorder of the young population with an age range of 17–25 years, however the incidence was reported to be less common in younger children, with approximately 300 cases since its initial discovery [11,12]. Since this study was conducted in the pediatric age group, the patients were already at a higher risk of developing UPS, interestingly, the distribution of the cases favored the higher end of the age range between 13 to 18, which may be explained by the later stages of puberty. This age-related susceptibility is thought to be driven by androgen-mediated villous hair growth, which increases after puberty and leads to greater accumulation of hair and epithelial debris within the deep umbilicus [4]. Hair distribution and amount are thought to be another important risk factor with the hirsute individuals at a higher risk [3]. In the current study 29 patients (69%) had thick or dense body hair, which is similar to the previous studies conducted in wider age groups and in other or similar anatomical sites of PNS. Although males were the predominant sex in the literature to be affected by PNS generally and UPS specifically, and this increase in incidence in males could also be driven by androgen-based villous hair growth after puberty, at a set pattern and their higher incidence of hirsutism [4,10]. Yet in this study, the sex of the cases was nearly equally distributed with 22 (52.4%) males and 20 (47.6%) females with no significant differences in the amount of body hair.
Regarding weight and its relation with PNS, it is widely recognized in the literature that it is a significant risk factor, particularly in cases of sacrococcygeal PNS. In contrast, Coşkun et al. reported that obesity is not a risk factor for UPS, this may be the result of the flattening of umbilical hole in obese patients, hence decrease in the migration of hair in chest and abdominal area to umbilical hole [13]. However the cases in this paper had relatively high BMI, which might demonstrate an association between them, as also mentioned in a recent study that obesity is a risk factor for UPS by increasing skin creases, sweating and epithelial debris accumulation in the navel [4].
The relation between UPS and family history has been shown to be significant similarly in the current study one-third of the cases had relevant family history [9,13]. While other study done in similar age group on PNS in general has failed to find a relation [11], which might indicate a difference in the significance of family history between PNS in general and UPS. Umbilical pilonidal sinus is demonstrated to be more prominent among students [5]. Similar to this, the current study predominantly comprises students, this distribution may not necessarily indicate a direct association, as UPS is more prevalent among younger individuals, a demographic that largely overlaps with the school-age population.
Wearing belt has been theorized to be a possible risk factor for UPS, with the hypotheses of the umbilicus being on the belt line where clothes fit tightly and twisting of the trunk occurs, thereby increasing the risk of friction between hairs and the umbilicus predisposing hairs to getting caught, also wearing belt causes the hairs to be collected at the level of umbilicus and sets the ground for a moist environment, with the hairs piercing the skin, yet other studies failed to find an association [3,13]. Although most cases in the present study reported belt use (69.0%), this difference is not considered sufficient to demonstrate statistical significance.
Due to the rarity of UPS and the possibility of other differential diagnosis, like umbilical hernia, Umbilical granulomas, metastatic tumors like Sister Mary Joseph nodule, omphalomesenteric duct remnants (Meckel’s diverticulum), urachal anomalies, endometriosis in women, nevi and sometimes rare but important aggressive tumors like basal cell carcinoma, there is a need for well-defined diagnostic criteria. Furthermore, presenting symptoms should be clearly characterized, along with their implications for diagnosis, management, and clinical outcomes [12,14]. The findings of this study show that the most common presenting symptoms was the presence of discharge which was 35 cases (83.3%) followed closely by pain which was 34 cases (81.0%) which is similar to the literature with the pain and discharge being the most reported symptoms with itching also being a common presenting symptom. It is important to note that in this study patients with a lower BMI were significantly more likely to present with purulent discharge while itching was more common in those with a higher BMI, presence of swelling was associated with the presence of sinus opening but number of the sinuses and the presence of granuloma or abscess could not be associated to the presenting symptoms and those with longer duration of symptoms were more likely to complain of itching compared to other symptoms [2,4,5].
The management of UPS remains controversial, with no established consensus on the optimal treatment approach [1]. The rarity of UPS means that high-level clinical evidence comparing different modalities is lacking, and most published data consist of case reports and small case series, several studies have reported successful outcomes with conservative, non-operative methods, including local hair removal, sinus cleaning, and the application of various agents [5,15]. Conversely, other research has demonstrated the superiority of surgical intervention over conservative treatment, particularly regarding long-term cure and recurrence rates [1]. More recently, umbilicus preserving surgical techniques have been proposed as an alternative to complete omphalectomy, aiming to achieve low recurrence while maintaining acceptable cosmetic results [2].
Although conservative approaches are simple to do and inexpensive, the sensitive skin of the umbilicus remains a risk for future recurrence, while the recurrence rate is between 4.4% and 27.0% and the healing rate is between 100% and 78.6%, depending on the type of conservative treatment that is used. Surgery, however, appears to be more successful in UPS. It reduces the depth of the navel, which reduces the unfavorable pressures in the umbilicus and so prevents recurrences more efficiently than conservative therapy. Several surgical approaches have been proposed in the literature, including complete excision of the sinus and reconstruction, excision and laying open, omphalectomy through a transverse incision and primary suture under general anesthesia, omphalectomy with plastic reconstruction, and excision of the cavity through a supraumbilical incision and curetting, with the recurrence rate of the surgical treatment being (2.5%) and the healing rate being (100%) [1,5]. The recurrence rate is comparable to the present study which was (2.4%), but the healing rate was (95.2%).
This study is limited by its single-center design, which may restrict the generalizability of the findings. In addition, the relatively small sample size may have reduced the statistical power of the analysis. Furthermore, reliance on patient-reported variables may have introduced reporting bias.
Conclusion
Surgical management demonstrated favorable outcomes, with high healing rates and low recurrence, supporting its role as an effective treatment modality in pediatric patients. Given the absence of standardized guidelines, further larger, multicenter studies are required to better define risk factors and establish optimal management strategies for this condition.
Declarations
Conflicts of interest: The authors have no conflicts of interest to disclose.
Ethical approval: In accordance with our institution's oral policy, retrospective cohort studies involving anonymized histopathological material and de-identified patient data do not require formal ethical approval.
Patient consent (participation and publication): Informed consent was obtained from all patients for the use of their clinical data and for publication.
Funding: The present study received no financial support.
Acknowledgements: None to be declared.
Authors' contributions: ISS, OAA, AOH, DAK, SHA and IRR were significant contributors to the conception of the study, the literature search for related studies, managed the cases, and performed critical revision. AMS and AAQ contributed to the conception of the idea, data collection and interpretation, and critical revision. MBA, KKM, HAH and KAN contributed to the conception of the idea, literature review, table preparation, and critical revision. AKM contributed to the conception of the idea, literature review, and drafting of the manuscript. All authors have read and approved the final version of the manuscript.
Use of AI: ChatGPT-4.5 was used to assist with language refinement and improve the overall clarity of the manuscript. All content was thoroughly reviewed and approved by the authors, who bear full responsibility for the final version.
Data availability statement: The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
- Kaplan M, Ozcan O, Kaplan FC, Yalcin HC, Salman B. Conservative vs surgical interventions for umbilical pilonidal sinus: a multicenter, double-blind, prospective, randomized clinical trial. Journal of the American College of Surgeons. 2016;222(5):878-89. doi:10.1016%2Fj.jamcollsurg.2016.01.056
- Tendulkar SP, Jain PA, Mehta MG. Umbilical Pilonidal Sinus and Role of Umbilicus Preserving Surgery. Indian Journal of Colo-Rectal Surgery. 2025;8(1):30-2. doi.org/10.4103%2Fijcs.ijcs_1_25
- Othman B, An V. Umbilical pilonidal sinus: a rare cause of umbilical discharge. ANZ Journal of Surgery. 2022;92(12):3371. doi:10.1111/ans.17691
- Bamalan OA, Alsubeai HS, Hijazi FT, Almohaisin AA, Bubshait AS, Alnasser AH, et al. Umbilical Pilonidal Sinus: a Case Report and Systematic Review. Medical Archives. 2025;79(5):417. doi:10.5455/medarh.2025.79.417-427
- Muhialdeen AS, Baba HO, Salih AM, Fathalla BL, Latif S, Hasan SJ, et al. Non‐operative management of umbilical pilonidal sinus: One more step towards ideal therapy. International Wound Journal. 2023;20(7):2505-10. doi:10.1111/iwj.14111
- Muhialdeen AS, Ahmed JO, Baba HO, Abdullah IY, Hassan HA, Najar KA, et al. Kscien’s list: a new strategy to discourage predatory journals and publishers (second version). Barw Med J. 2023;1(1):24–26. doi:10.58742/bmj.v1i1.14
- Memisoglu E. Predisposing factors for failure of conservative treatment in umbilical pilonidal sinus: A clinical experience; Annals of Medical Research. 2019;26(10):2105-9. doi:10.5455/annalsmedres.2019.07.367
- Siddiq ES, Hassan SH, Qadir AA, Abdulkarim MM, Qader IH, Hamad KZ. Multiple Concurrent Pilonidal Sinuses: Case report and Literature review. Judi Clinical Journal. 2025;1(1):67-70. doi:10.70955/JCJ.2025.8
- Isik A, Wysocki AP, Memiş U, Sezgin E, Yezhikova A, Islambekov Y. Factors associated with the occurrence and healing of umbilical pilonidal sinus: a rare clinical entity. Advances in Skin & Wound Care. 2022;35(8):1-4. doi:10.1097/01.ASW.0000833608.27136.d1
- Salih AM, Kakamad FH, Muhialdeen AS, Zahir HM, Saeed YA, Ali HO, et al. Co-occurrence of posterior chest wall pilonidal sinus with melanocytic nevus: a challenging presentation: a case report. Journal of Cardiothoracic Surgery. 2024;19(1):330. doi:10.1186/s13019-024-02802-y
- Faraj FH, Baba HO, Salih AM. Risk factors of pilonidal sinus disease in preparatory school students; a case control study. Annals of Medicine and Surgery. 2020 Sep 1;57:46-8. doi:10.1016/j.amsu.2020.07.016
- Hsu L, Lesher AP. Umbilical pilonidal sinus in a teenager: A case report. Journal of Pediatric Surgery Case Reports. 2023;93:102631. doi:10.1016/j.epsc.2023.102631
- Coşkun A, Buluş H, Faruk Akıncı Ö, Özgönül A. Etiological factors in umbilical pilonidal sinus. Indian Journal of Surgery. 2011;73(1):54-7. doi:10.1007%2Fs12262-010-0226-x
- Salih AM, Kakamad FH. Basal cell carcinoma mimicking pilonidal sinus: a case report with literature review. International journal of surgery case reports. 2016;28:121-3. doi:10.1016/j.ijscr.2016.09.040
- Salih AM, Ahmed MM, Baba HO, Kakamad FH, Salih KM, Muhedin SS, et al. Non‐operative management of pilonidal sinus disease; classification and outcome. International Wound Journal. 2023;20(9):3639-47. doi:10.1111/iwj.14242

This work is licensed under a Creative Commons Attribution 4.0 International License.