

Volume 4, Issue 1, 2026
PublishedJune 2026
Published
June 30, 2026
Original Articles
Introduction
Alzheimer's disease (AD) is the most common neurodegenerative cause of dementia. Social media has become a major source of information for patients and families. This study is the first to explore the quality, source, and content of AD videos on TikTok with emphasis on the role of healthcare professionals (HCPs).
Methods
A cross-sectional analysis was conducted on April 30, 2025, on AD videos on TikTok, including the data of usernames, video title, date of posting, and days since uploaded, video duration, video sources or uploader, content type, and engagement metrics. The DISCERN tool, a 15-item questionnaire for judging the quality of written consumer health information on treatment choices, was used to evaluate the quality of health information. Statistical analysis was conducted using R Statistical software.
Results
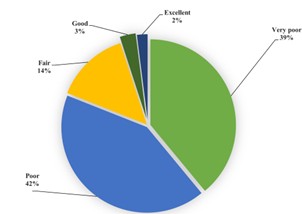
In total, 100 videos of the hashtag Alzheimer's were deemed eligible with median (interquartile range) engagement metrics: 4201.00 (300.25 to 66775.00) likes, 131.50 (13.00 to 1071.00) comments, and 438.00 (43.00 to 3414.00) shares. HCPs streamed only 33% of videos. There were videos about therapy suggestions (10%), disease descriptions (30%), and lifestyle (16%). The majority had poor (42%) and very poor (39%) quality. Videos by HCPs had more medical content with higher quality despite insignificant differences in engagement compared to non-HCP videos.
Conclusion
This study revealed an overall poor quality of public information on AD on TikTok, with a paucity of essential information, with minor contributions from HCPs. HCPs and organizations should provide creative, systematic plans to enhance public awareness on social media.
Introduction
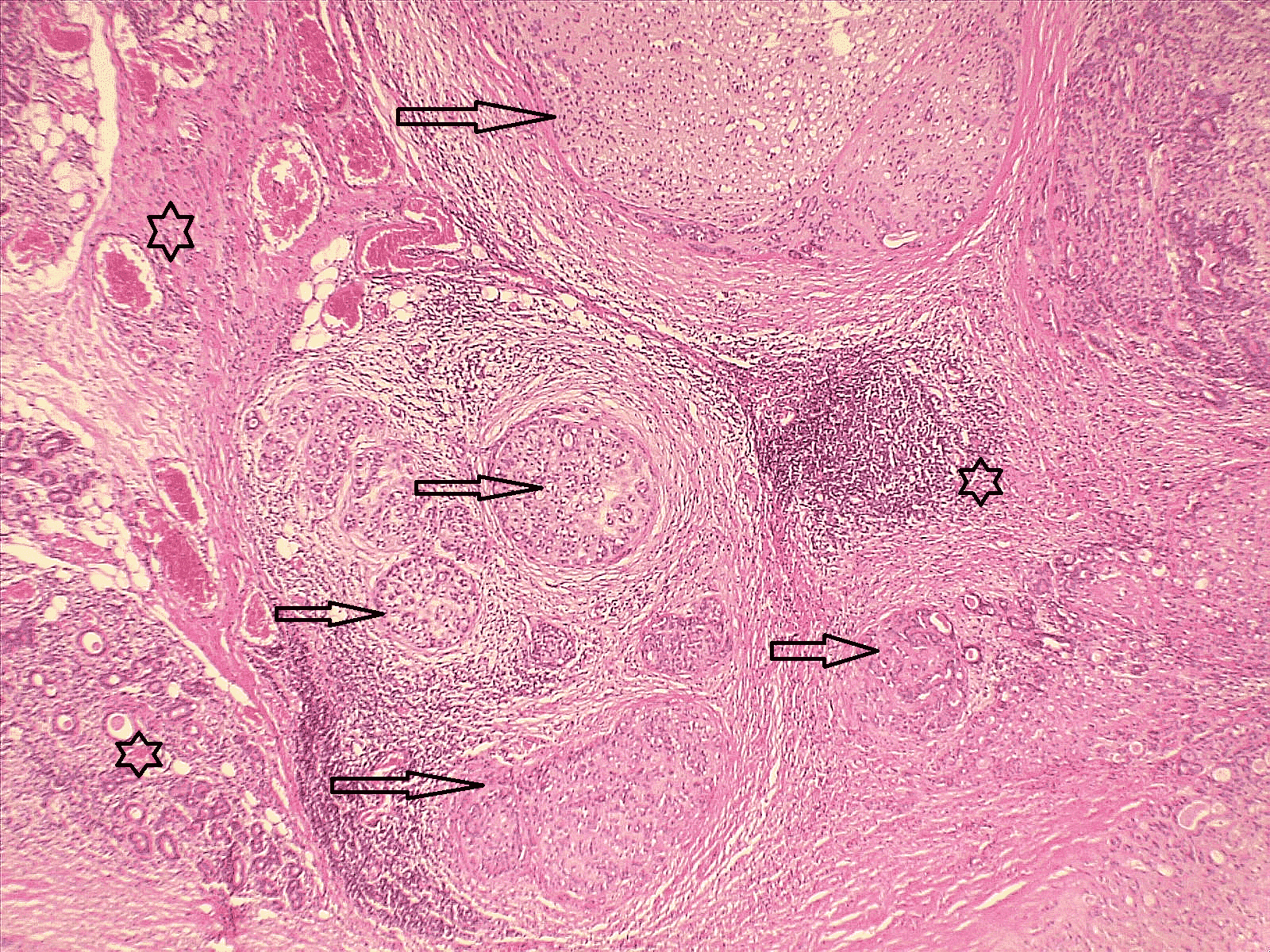
Epithelial-myoepithelial carcinoma (EMC) is a rare, biphasic malignant tumor affecting the salivary glands. It represents less than 1% of all salivary gland tumors. This study aims to present a single-center experience regarding the diagnosis, management, and prognosis of EMC.
Methods
This study was conducted between February 2020 and December 2025. Patients with a histopathologically confirmed diagnosis of epithelial-myoepithelial carcinoma were identified. Complete medical records containing demographics, clinical presentation, imaging results, histological features, treatment approaches, and follow-up results were included in the cases.
Results
Five patients were identified, of which 4 (80%) were females. The mean age was 56 ± 9.38 years. Two patients (40%) presented with painless post-auricular swelling, 1 (20%) with submandibular swelling, and 2 (40%) were incidental findings. Histopathological examination confirmed EMC in all cases. Free margins were achieved in 3 tumors (60%). No recurrence was observed during a mean follow-up of 24 ± 28.92 months.
Conclusion
Epithelial-myoepithelial carcinoma is a very rare tumor. It requires histopathological evaluation for accurate diagnosis, and complete surgical excision offers favorable short-term outcomes. Further studies are needed to better define its clinical characteristics and outcomes.
Introduction
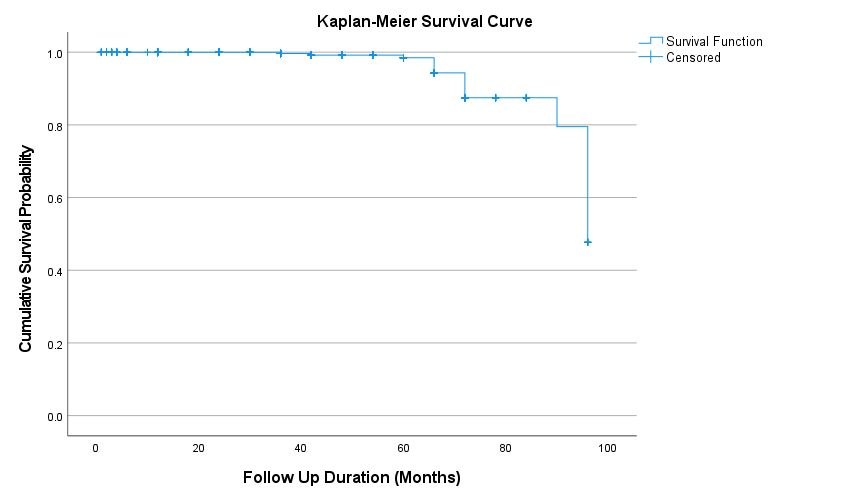
Breast cancer in young women, defined as diagnosis before 40 years of age. It is characterized by poorer outcomes compared with older patients. Regional data on the disease in the Middle Eastern population remain limited. This study focused on the clinicopathological profile of young women with breast cancer.
Methods
This retrospective, single-center cohort study was conducted between February 2018 and February 2025. Demographic, clinical, pathological, treatment, and follow-up data were extracted from electronic medical records. Inclusion criteria were women under 40 years diagnosed with primary breast cancer. Patients with incomplete records or without surgical treatment were excluded.
Results
A total of 564 patients with a median age of 36 years (IQR: 5) were included. A breast mass was the predominant chief complaint (85.5%), and 74.7% presented within 3 months. Median tumor size was 25 mm. Invasive ductal carcinoma was the predominant subtype (88%). Triple-negative breast cancer was identified in 73 patients (12.9%), of which 76.1% were Grade III (p<0.001). Negative estrogen and progesterone receptor status was significantly associated with Grade III (p<0.001). Wide local excision was performed in 67.0% of cases. Overall survival was 98.5% at 60 months.
Conclusion
High tumor grade was significantly associated with triple negative breast cancer, ER-negative, and PR-negative status, but not with HER2 status. Symptom duration showed no association with tumor size. Ki-67 was significantly higher in Grade III tumors, reinforcing the aggressive phenotype of breast cancer in young women
Introduction
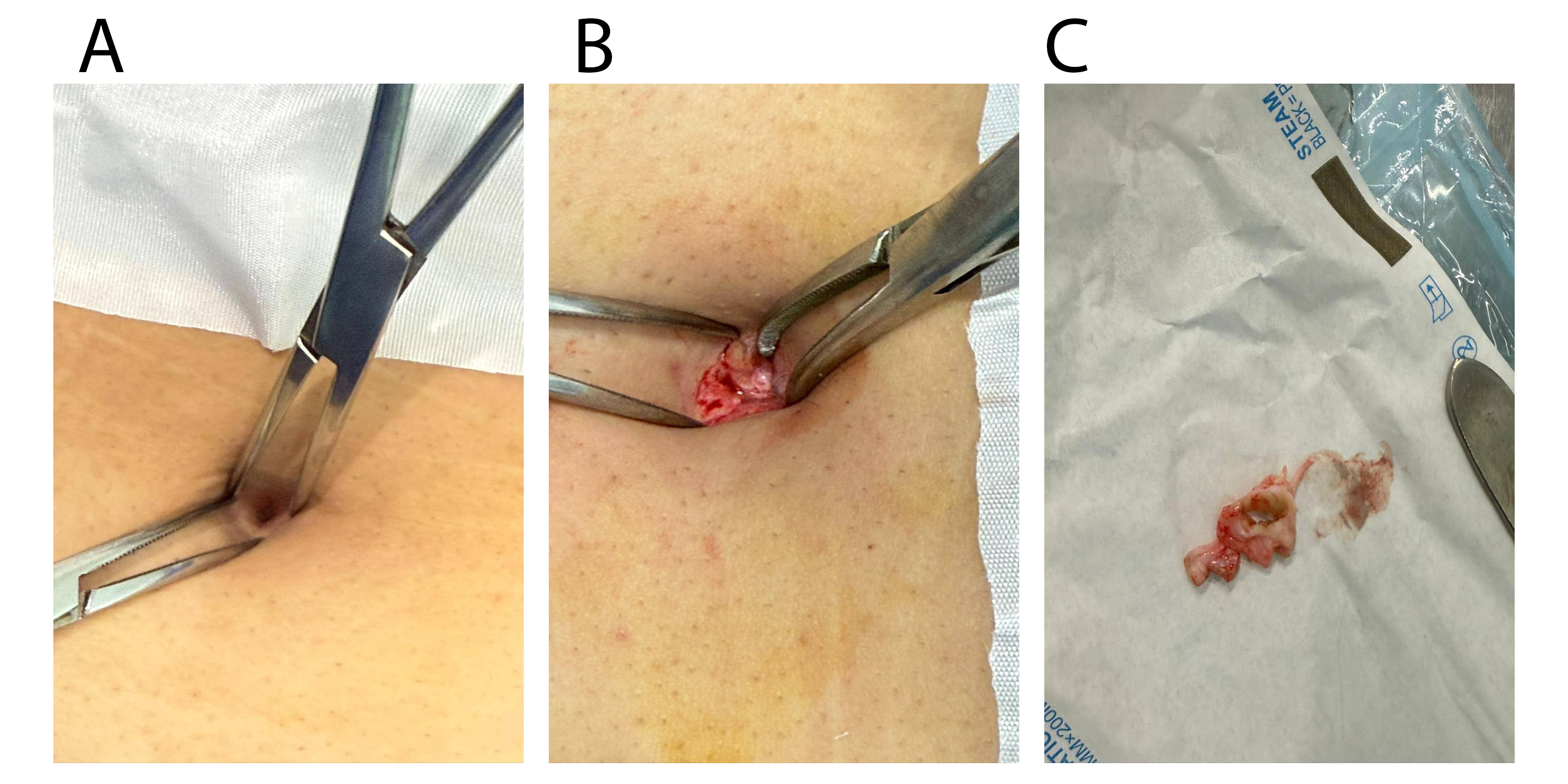
Umbilical pilonidal sinus (UPS) is a rare form of pilonidal disease (PNS) predominantly affecting young individuals. Owing to its low incidence, data on risk factors and optimal management remain limited. This study aimed to investigate UPS in the pediatric age group and evaluate the efficacy of surgical management.
Methods
A retrospective, single-center cohort study was conducted over five years, including patients aged ≤18 years diagnosed with UPS. Clinical, demographic, and risk factor data were collected from medical records. All patients underwent surgical management under local anesthesia, with follow-up to assess healing and recurrence. Descriptive statistical analysis was performed using SPSS version 27.0.
Results
A total of 42 cases (mean age 16.4 ± 1.48 years) were included. Males comprised 22 (52.4%) of cases. Dense body hair was observed in 29 (69.0%) of patients, and 15 (35.7%) reported a positive family history, and obesity was common (median body mass index (BMI) was 25.9 (IQR: 22.5–29.0)). Surgical treatment achieved successful healing in 40 (95.2%) of cases, with a low recurrence rate of 1 (2.4%).
Conclusion
Surgical management showed favorable outcomes with high healing and low recurrence rates, supporting its effectiveness in pediatric patients. However, larger multicenter studies are needed to clarify risk factors and optimize management strategies
The rapid growth of open access publishing (OAP) has significantly improved the accessibility and dissemination of scientific knowledge. However, this expansion has also contributed to the emergence of non-recommended journals (NRJs) and non-recommended publishers (NRPs) that exploit researchers by offering rapid publication without maintaining proper peer-review standards. Such practices threaten the credibility of scholarly communication and may lead to the dissemination of low-quality or unreliable research. In response to this challenge, several initiatives have developed lists and monitoring systems to help researchers identify potentially NRJs. This study reviews major NRPs and NRJs evaluation platforms, including Beall’s List, Cabells’ Predatory Reports, Kscien’s List, Predatory Reports, Academic Journal Predatory Checking (AJPC), the Early Warning List of International Journals, Kanalregister, the Open Access Journal List, the Journal Insights Predatory List, and the International Journals Blacklist. The review examines their objectives, operational approaches, strengths, and limitations in identifying deceptive publishing practices. The findings indicate that while these lists serve as useful preliminary screening tools, they vary in transparency, accessibility, evaluation criteria, and governance structures. Some rely on expert assessment, whereas others apply automated or bibliometric methods. Despite their usefulness, no single list can comprehensively identify all NRJs, and misclassification may occur. Therefore, researchers should use these tools cautiously and combine them with independent evaluation of journal credibility to ensure responsible publishing and maintain the integrity of scientific communication.
Introduction
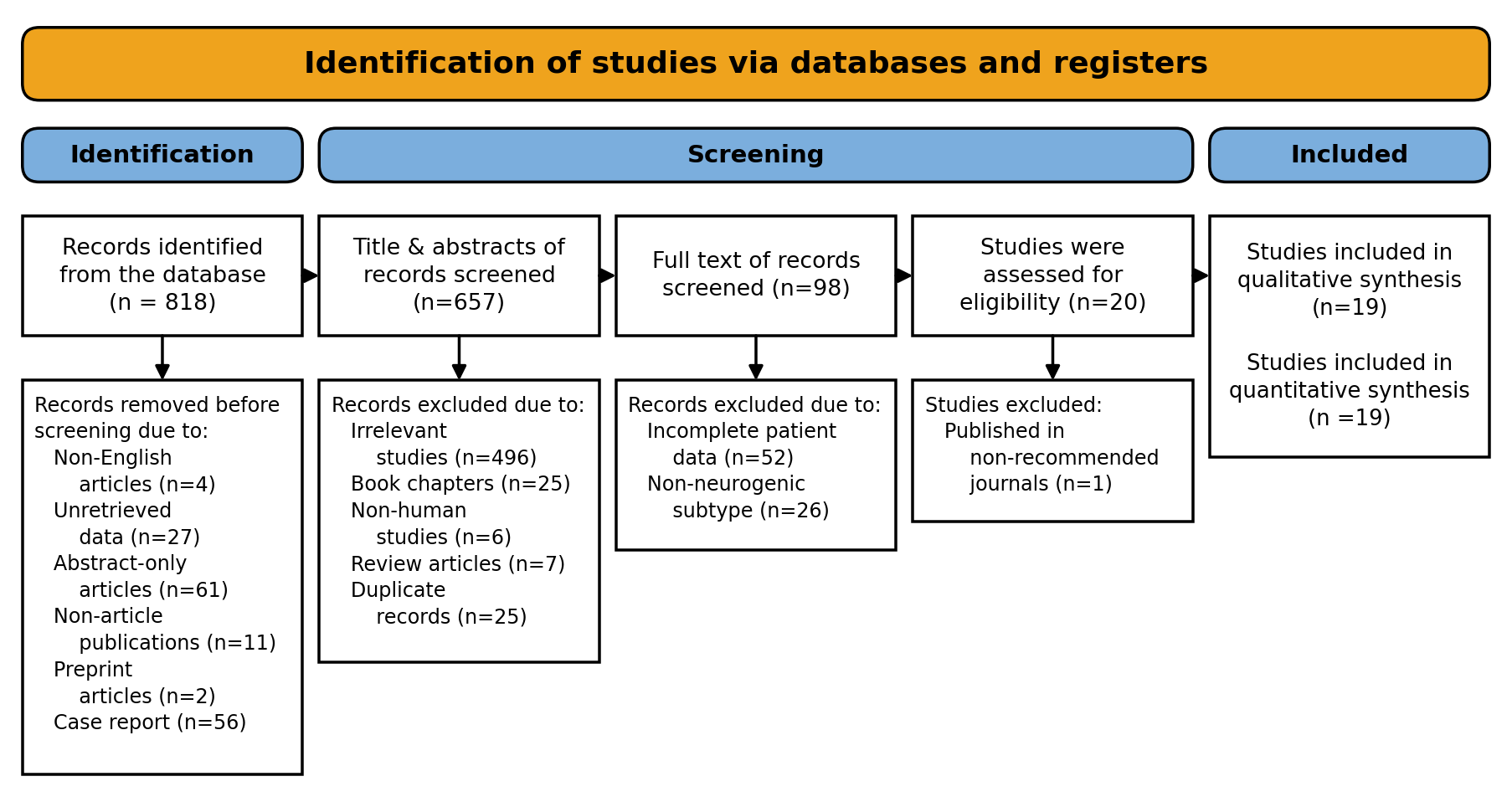
Neurogenic thoracic outlet syndrome (NTOS) is the most common subtype of thoracic outlet syndrome and results from compression of the brachial plexus within the thoracic outlet. First rib resection (FRR) is considered the cornerstone of surgical management in patients with refractory symptoms, although postoperative outcomes remain variably reported. This systematic review aimed to evaluate the outcomes, complications, and recurrence rates of FRR in the management of NTOS.
Methods
A systematic review was conducted using Google Scholar, supplemented by artificial intelligence-assisted searches. Original studies reporting postoperative outcomes following FRR for NTOS were included. Data regarding patient characteristics, surgical approaches, postoperative outcomes, complications, and recurrence were extracted and analyzed descriptively. Comparative analyses between surgical approaches were performed using Chi-square testing.
Results
Nineteen studies involving 1,334 operated sides were included. Most studies were cohort studies (73.68%). Females represented 75.44% of reported patients. Successful postoperative outcomes were observed in 87.08% of analyzable cases. No statistically significant difference in success or recurrence rates was identified between the open approaches. A total of 170 complications were recorded among operated sides managed via the transaxillary approach. Pneumothorax was the most frequently reported complication in both the transaxillary (n = 99, 20.58%) and supraclavicular (n = 7, 2.68%) approaches. The overall recurrence rate was 1.50%.
Conclusion
First rib resection is a safe and effective surgical intervention for NTOS, yielding favorable outcomes with low recurrence across a broad range of operative approaches. Neither the choice of surgical approach nor the extent of rib resection significantly influences surgical success.
Introduction
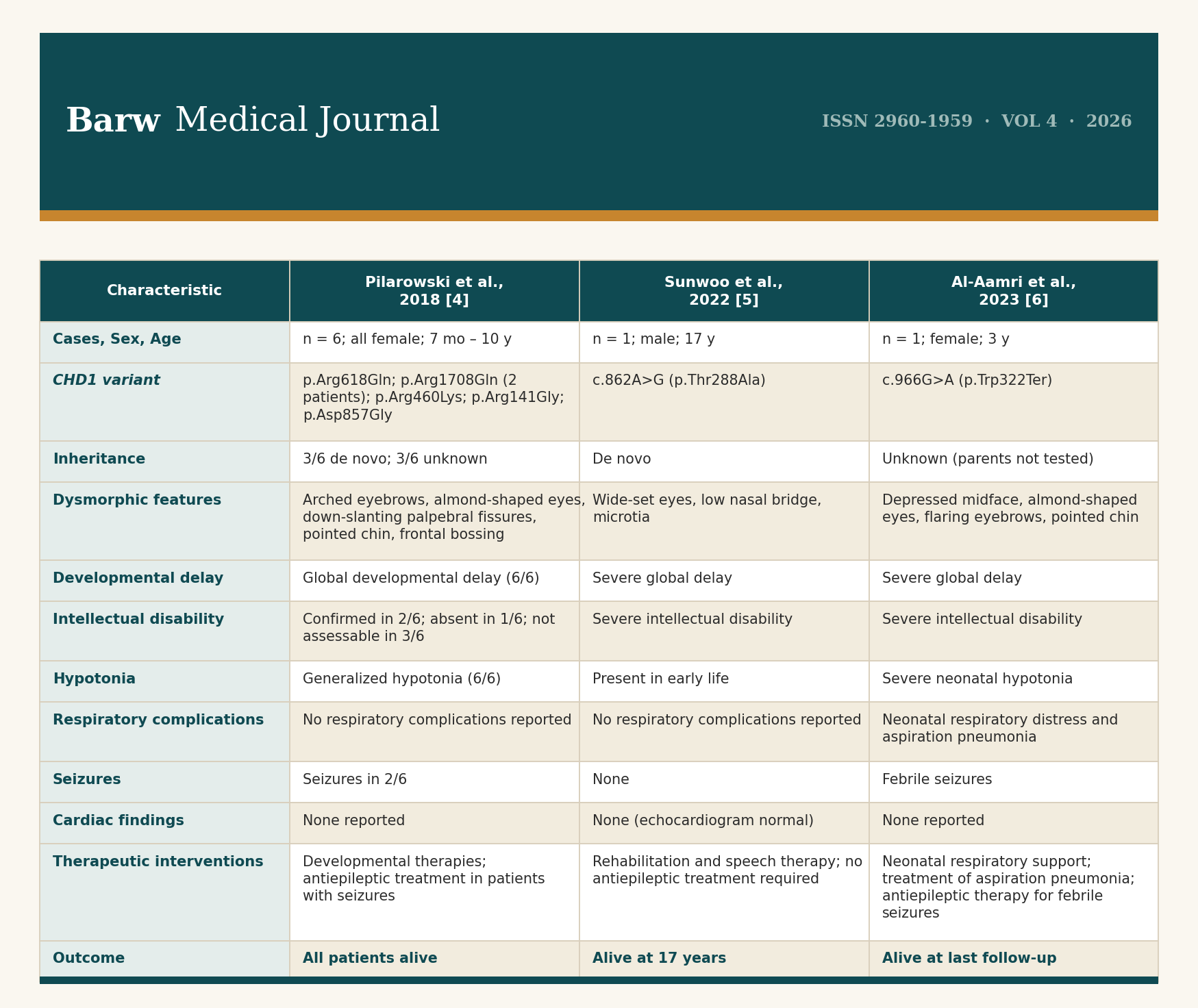
Pilarowski–Bjornsson syndrome (PILBOS) is a rare autosomal dominant neurodevelopmental disorder caused by heterozygous variants in chromodomain helicase DNA-binding protein 1 (CHD1), a gene encoding an adenosine triphosphate (ATP)-dependent chromatin remodeler. Since its initial description in 2018, only a limited number of cases have been reported in the literature.
Case Presentation
A 4-month-old male infant presented with persistent hypotonia and recurrent focal seizures beginning in the neonatal period, accompanied by severe global developmental delay. Brain magnetic resonance imaging (MRI) was structurally normal. Whole exome sequencing identified a heterozygous de novo CHD1 variant (NM_001270.4: c.797C>T; p.Pro266Leu), classified as a variant of uncertain significance. Echocardiography revealed a medium-sized secundum atrial septal defect with right-sided chamber dilatation. The clinical course was complicated by recurrent lower respiratory tract infections and progressive respiratory distress.
Literature Review
Review of eight previously reported cases confirms global developmental delay and hypotonia as universal features of PILBOS (8/8, 100%). Dysmorphic craniofacial findings were present in 7/8 (87.5%) cases, and seizures occurred in 3/8 (37.5%). Intellectual disability was confirmed in 3/8 (37.5%) and not assessable in a further 3/8 (37.5%). Respiratory complications were documented in 1/8 (12.5%) cases. De novo inheritance was confirmed in 4/8 (50%) cases. No structural cardiac defects have been documented in any previously reported case, and all 8/8 (100%) patients were alive at last follow-up.
Conclusion
Findings from this case suggest that structural congenital heart defects may represent an underrecognized component of the PILBOS phenotypic spectrum. Further case reports and functional investigations are required to establish whether cardiac involvement constitutes a consistent feature of CHD1-related disease.
Introduction
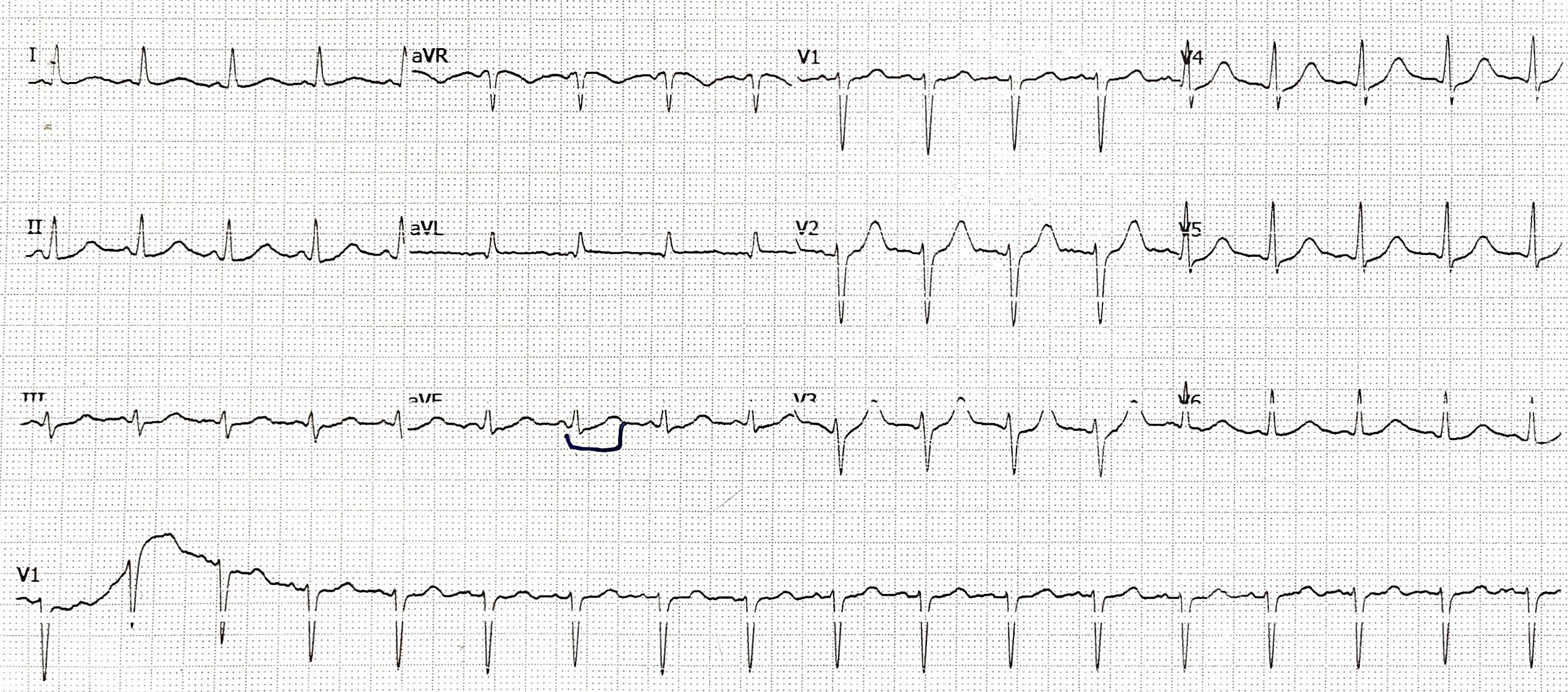
Ondansetron blocks human ether-à-go-go-related gene (hERG) potassium channels, causing QT prolongation and risk of torsades de pointes (TdP). Despite its widespread use, TdP following a standard intravenous dose is rarely reported. This report presents a case of a 40-year-old female who developed TdP after receiving an 8 mg intravenous dose of ondansetron.
Case Presentation
A 40-year-old female with no significant past medical history presented with vomiting and diarrhea. Approximately 30 minutes after receiving 8 mg of intravenous ondansetron, she developed TdP requiring cardioversion. Laboratory results revealed mild hypokalemia (3.12 mmol/L). Post-event troponin elevation and Grade I diastolic dysfunction suggested transient myocardial involvement. She was stabilized with potassium replacement and supportive care, with full recovery.
Literature Review
Five cases of ondansetron-induced TdP were reviewed. Patient ages ranged from 41 to 60 years, one case (20%) involved oral administration and four cases (80%) involved intravenous administration. Doses ranged from standard 4 mg to cumulative 36 mg infusions, with QTc intervals reaching up to 653 ms. Presenting events included TdP, ventricular tachycardia, and cardiac arrest. Symptom resolution and recovery were achieved in all cases following medical intervention and electrolyte correction.
Conclusion
This case highlights that standard-dose ondansetron can precipitate TdP in physiologically unstable patients.
Dear Editor,
The issue raised by Tiesenga et al. [1], namely of the nomenclature used to characterize a journal or publisher as “predatory” or otherwise, has been previously debated to some extent [2]. The issue of predatory versus exploitative behavior in academic publishing is also a well-explored debate [3]. Furthermore, the grey zone between what constitutes “predatory” behavior and what this term does not encompass is expanding because several journals and publishers that were once considered safe to publish in, having conducted peer review and ranked by metrics, have failed their own stated quality standards [4], as evidenced by the growth in retraction rates in some of those journals and publishers) [5]. Therefore, several of the issues debated by Tiesenga et al. [1] have already been debated, even though relevant literature was not cited. The originality of the core proposal by Tiesenga et al. is also in question since, as indicated in entry #9 of Table 2 in their article, the European Association of Science Editors had already recommended a shift in the term “predatory” to “non-recommended” in 2025.
On page 36, section 4.2 of Tiesenga et al. [1], the Kscien predatory publishing lists are advertised. Kscien – with which the article’s corresponding author is affiliated – is an organization based in Iraq that has, since 2017, emerged as a replacement to Beall’s original blacklists. One problem with the Kscien blacklist is that it classified – when this letter was originally written – 3539 entities as being “predatory”, a label that directly contradicts the core argument of their article, which advocates that the term “predatory” should not be used. This contradictory stance by Kscien related to use of the term “non-recommended” as opposed to “predatory” is emphasized by the authors’ statement on page 39, where it states that “One clear advantage of the term “predatory” is its moral precision and clarity because it explicitly signals condemnation of exploitative publishing practices and conveys the seriousness of their questionable and unethical practices.” In other words, according to this definition, the Kscien “predatory publishing” blacklist is certain about the predatory nature of the 3539 entities, even though Kscien provides no tangible evidence to support that classification.
Tiesenga et al. define their paper’s objective on page 35, namely to adopt “more neutral language that can help to protect academic integrity while reducing legal and reputational risks”, although no evidence is provided that academic integrity will be protected, nor that legal and reputational risks will be reduced, simply by changing the label of a journal or publisher from “predatory” to “non-recommended”. Ultimately, a veritable threat can be euphemistically referred to as “risky” but if the threat to scientific integrity is real, it will impact all academics, including those that employ euphemistic language and those that employ straightforward and unambiguous terms to define the threat. If evidence of “predatory” publishing behavior is clear and unambiguous, then freedom of speech will not be threatened.
“Renaming the problem: Why ‘non-recommended journals’ is preferable to ‘predatory’ in academic publishing” Barw Medical Journal. 2025;3(5):33-41.
Following correspondence received by the editorial office regarding authorship confirmation and reference accuracy, the journal conducted an editorial review in accordance with the guidance of the Committee on Publication Ethics.
Authorship correction
During this process, two individuals listed as authors informed the journal that they had not approved the final version of the manuscript prior to submission. After communication with the corresponding author and available co-authors, the authorship list has been revised accordingly. The corrected author list is provided below.
Corrected author list:
Frederick M. Tiesenga, Daniel Rodger, Benjamin Saracco, Baichang Zhong, Andrea Cortegiani, Sjaak Pouwels, Rawezh Qadir M. Salih, Ayman M. Mustafa, Michele Meoli, Svitlana Fiialka, Khritish Swargiary, Purvi Raj Bhagat, Suad Kunosic, Rosa Rodriguez-Sánchez, Kaushik Bhattacharya, Marco Cascella, Mohmedhanif Nashipudi, Bharat Gurnani, Kirandeep Kaur, P. Paramashivaiah, B.T Sampath Kuma, Givheart Dano, Mallikarjun Dora, Bolaji David Oladokun, Manzoor V. Babu, AR. Saravanakumar, Usman Muhammed Song, Vemma Mae R. Guinto, Karthik N. Rao, Alireza Akbari, Arslan Sheikh, Punnya Angadi, Johnkennedy Nnodim, Jafaru Aliyu Shinkafi, Sanjeev Rastogi, Kunle Oparinde, Klimis Ntalianis, Saeeda Abdullah, Atanu Chandra, Collence Chisita, Mohd Amzari Tumiran, Haneen Ali Haleem, Harsh Deora
Reference correction
Reference number 28 cited an article that has since been deleted as it was a duplicate (not retracted). This reference has been replaced by its original one: Kakamad F. H., Mohammed S. H., Najar K. A., Qadr G. A., Ahmed J. O., Mohammed K. K., et al. Kscien's list; a new strategy to discourage predatory journals and publishers. International Journal of Surgery Open. 2019, 23, 54-56. https://doi.org/10.1016/j.ijso.2019.11.001
These corrections do not affect the scientific content or conclusions of the article. The original article remains unchanged, and readers are advised to consult this notice for the corrected information.