
Surgical Outcomes Following First Rib Resection for Neurogenic Thoracic Outlet Syndrome: A Systematic Review of 1,334 Operated Sides

Abstract
Introduction
Neurogenic thoracic outlet syndrome (NTOS) is the most common subtype of thoracic outlet syndrome and results from compression of the brachial plexus within the thoracic outlet. First rib resection (FRR) is considered the cornerstone of surgical management in patients with refractory symptoms, although postoperative outcomes remain variably reported. This systematic review aimed to evaluate the outcomes, complications, and recurrence rates of FRR in the management of NTOS.
Methods
A systematic review was conducted using Google Scholar, supplemented by artificial intelligence-assisted searches. Original studies reporting postoperative outcomes following FRR for NTOS were included. Data regarding patient characteristics, surgical approaches, postoperative outcomes, complications, and recurrence were extracted and analyzed descriptively. Comparative analyses between surgical approaches were performed using Chi-square testing.
Results
Nineteen studies involving 1,334 operated sides were included. Most studies were cohort studies (73.68%). Females represented 75.44% of reported patients. Successful postoperative outcomes were observed in 87.08% of analyzable cases. No statistically significant difference in success or recurrence rates was identified between the open approaches. A total of 170 complications were recorded among operated sides managed via the transaxillary approach. Pneumothorax was the most frequently reported complication in both the transaxillary (n = 99, 20.58%) and supraclavicular (n = 7, 2.68%) approaches. The overall recurrence rate was 1.50%.
Conclusion
First rib resection is a safe and effective surgical intervention for NTOS, yielding favorable outcomes with low recurrence across a broad range of operative approaches. Neither the choice of surgical approach nor the extent of rib resection significantly influences surgical success.
Introduction
Thoracic outlet syndrome (TOS) refers to a group of disorders caused by compression of neurovascular structures traversing the thoracic outlet. Depending on the affected structure, TOS is classified into neurogenic, venous, and arterial subtypes, corresponding to compression of the brachial plexus, subclavian vein, and subclavian artery, respectively [1,2]. Neurogenic thoracic outlet syndrome (NTOS) is the predominant form, accounting for approximately 90%–95% of all cases, whereas venous and arterial TOS represent approximately 3%–5% and 1%, respectively [3–5]. Neurogenic TOS is further categorized into true and disputed forms, with disputed NTOS reportedly constituting 95%–99% of neurogenic cases [6].
The estimated annual incidence of NTOS is 2–3 cases per 100,000 population, with a point prevalence of approximately 10 per 100,000 individuals [7,8]. The underlying pathophysiology most commonly involves compression of the brachial plexus, particularly the inferior trunk, which originates from the C8–T1 nerve roots, within the scalene triangle or the costoclavicular space [6].
The etiology of TOS is multifactorial and may be congenital, traumatic, or functionally acquired. Congenital causes include anatomical abnormalities such as cervical ribs and anomalous first ribs. Traumatic etiologies most commonly involve whiplash injuries and falls, whereas functionally acquired forms are associated with repetitive upper extremity activities related to occupation or athletic performance [2,6,9].
The diagnosis of NTOS remains challenging in contemporary clinical practice. No single investigation is considered diagnostic, and the condition is primarily identified through clinical evaluation based on symptomatology, provocative physical examination maneuvers, and exclusion of alternative diagnoses such as cervical radiculopathy, peripheral nerve entrapment syndromes, and other structural abnormalities [8,10,11].
Conservative management is considered the initial treatment strategy for NTOS. Physical therapy programs focusing on postural correction, ergonomic modification, and stretching of the scalene and pectoralis minor muscles are generally recommended for at least four to six months before surgical intervention is considered. Adjunctive therapies, including local anesthetic injections, corticosteroids, and botulinum toxin, are also utilized in selected patients. Surgical decompression is typically reserved for individuals who fail nonoperative treatment [6,12–14].
First rib resection (FRR) is regarded as the cornerstone of surgical management for NTOS. Several operative approaches have been described, including supraclavicular, infraclavicular, and transaxillary techniques, with the choice of approach influenced by surgeon experience and patient-specific factors. More recently, minimally invasive techniques, including thoracoscopic-assisted and robotic approaches, have also been introduced into clinical practice [12,15,16].
The aim of this systematic review was to evaluate the postoperative outcomes of FRR in the management of NTOS, with particular emphasis on surgical success, complications, recurrence, and factors that may influence clinical outcomes across different operative approaches.
Methods
Study design
This study was conducted as a systematic review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. No prospective registration was performed prior to data collection.
Search strategy
A systematic literature search was conducted in Google Scholar using the keyword (first rib) with the allintitle function. This strategy was employed to maximize retrieval specificity for studies directly addressing the first rib as a primary subject. No time restriction was applied, and the search encompassed all records available up to the date of the final search (April 30, 2026). To supplement the primary database search and minimize the risk of missing relevant publications, additional searches were conducted using three artificial intelligence-based (AI-based) research tools: Consensus AI (consensus.app), Claude (Anthropic), and Perplexity AI (perplexity.ai). These platforms were queried using natural-language prompts, including "original studies reporting postoperative outcomes following first rib resection for neurogenic thoracic outlet syndrome". References identified through AI-assisted searching that were not retrieved by the primary Google Scholar search were cross-checked against the eligibility criteria and, where appropriate, retrieved in full text for screening. All records identified through AI tools were subject to the same inclusion and exclusion criteria as those identified through the primary database search. It is acknowledged that AI-assisted literature retrieval is not yet a standardized component of systematic review methodology; its use in this review was supplementary and intended to reduce retrieval bias rather than to replace conventional database searching.
Eligibility criteria
Studies were considered eligible for inclusion if they met the following criteria: (a) prospective or retrospective original research articles clearly reporting postoperative outcomes following FRR for NTOS; (b) studies utilizing any surgical approach or operative technique for FRR; and (c) studies reporting mixed TOS subtypes only when the data for NTOS patients were reported separately and could be extracted independently. The following records were excluded: (a) case reports; (b) studies with incomplete patient data or outcome information; (c) conference abstracts published without a full-text manuscript; (d) non-English language publications; (e) commentaries, letters to the editor, and editorial articles; (f) preprint publications; (g) studies focused on other subtypes of TOS; (h) studies reporting mixed TOS subtypes in which NTOS patients were not analyzed separately; (i) studies reporting exclusively on redo or revision surgical procedures; (j) studies in which only recurrence data were available without primary outcome reporting; (k) studies addressing anomalous FRR; and (l) studies published in non-recommended journals [17].
Study selection
Titles and abstracts of all retrieved records were independently screened against the predefined eligibility criteria. Full-text articles were subsequently retrieved for all potentially eligible studies, and a final inclusion decision was made following a detailed review of the complete manuscript.
Quality assessment
The methodological quality of the included studies was assessed according to study design. Cohort studies were appraised using the Newcastle–Ottawa Scale, which evaluates three domains: selection of study groups (maximum of four stars), comparability of groups (maximum of two stars), and ascertainment of outcomes (maximum of three stars), yielding a maximum score of nine stars. Studies scoring ≥7 stars were considered to have a low risk of bias; scores of 5–6 indicated a moderate risk, and scores ≤4 indicated a high risk of bias. Case series were evaluated using the Joanna Briggs Institute critical appraisal checklist for case series, which comprises 10 domains assessing methodological quality and reporting transparency. Each item was rated as “yes,” “no,” “unclear,” or “not applicable.” Studies scoring ≥8 were classified as low risk of bias, 5–7 as moderate risk, and ≤4 as high risk. The randomized controlled trials were assessed using the Cochrane Risk of Bias Tool version 2, which evaluates five domains: bias arising from the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in measurement of outcomes, and bias in selection of the reported results. Overall judgments were categorized as low risk, some concerns, or high risk of bias (Table S1).
Data extraction
Data were extracted using a standardized, predefined extraction form developed in Microsoft Excel. The following variables were extracted from each included study: (a) study characteristics, including first author, publication year, country of origin, study design, and number of participating centers; (b) patient demographics, including the number of patients with NTOS, number of operated sides, sex distribution, mean age, and age range; (c) surgical laterality, including unilateral versus bilateral procedures and right-sided versus left-sided procedures; (d) preoperative management details, including the duration and type of conservative treatment and preoperative botulinum toxin injection status; (e) operative details, including the surgical approach, type of rib resection performed, and mean operative time with range; (f) follow-up data, including mean follow-up duration and range; and (g) postoperative outcomes, including outcome grade, overall binary outcome (Successful/Failure), overall complication rate, specific postoperative complications, and recurrence.
Outcome standardization
Ordinal outcome classification
Due to variability in postoperative outcome reporting across the included studies, outcomes were standardized into a four-level ordinal classification system for data synthesis. When the original studies reported categorical or qualitative outcome descriptions, these were mapped as follows: (a) Excellent, defined as complete or near-complete resolution of symptoms with full return to pre-disease functional status and no requirement for ongoing treatment; (b) Good, defined as clear symptomatic improvement with minimal residual symptoms and no functional limitation in activities of daily living; (c) Fair, defined as partial symptomatic improvement with persistent complaints requiring ongoing conservative treatment or rehabilitation; and (d) Poor, defined as no improvement, worsening of symptoms, or the requirement for additional surgical or interventional procedures.
Binary outcome classification
Postoperative outcomes were additionally standardized into binary categories of successful and failure outcomes to allow comparability across studies with heterogeneous reporting systems. Outcomes described by the original authors as complete resolution, symptom resolution, marked improvement, good outcome, excellent outcome, or clinically meaningful improvement were categorized as successful outcomes. Outcomes described as persistent symptoms, no improvement, poor outcomes, treatment failure, or worsening symptoms were categorized as failure outcomes.
Statistical analysis
Descriptive statistics were used to summarize study characteristics, patient demographics, surgical variables, and postoperative outcomes. Continuous variables are reported as means with ranges where available. Categorical variables were reported as frequencies and percentages. Associations between categorical variables were analyzed using the Chi-square test. Crosstabulation analyses were performed in IBM SPSS Statistics (version 27.0; IBM Corp., Armonk, NY, USA). Statistical significance was assessed using the Pearson Chi-square test. A two-tailed P value of less than 0.05 was considered statistically significant.
Results
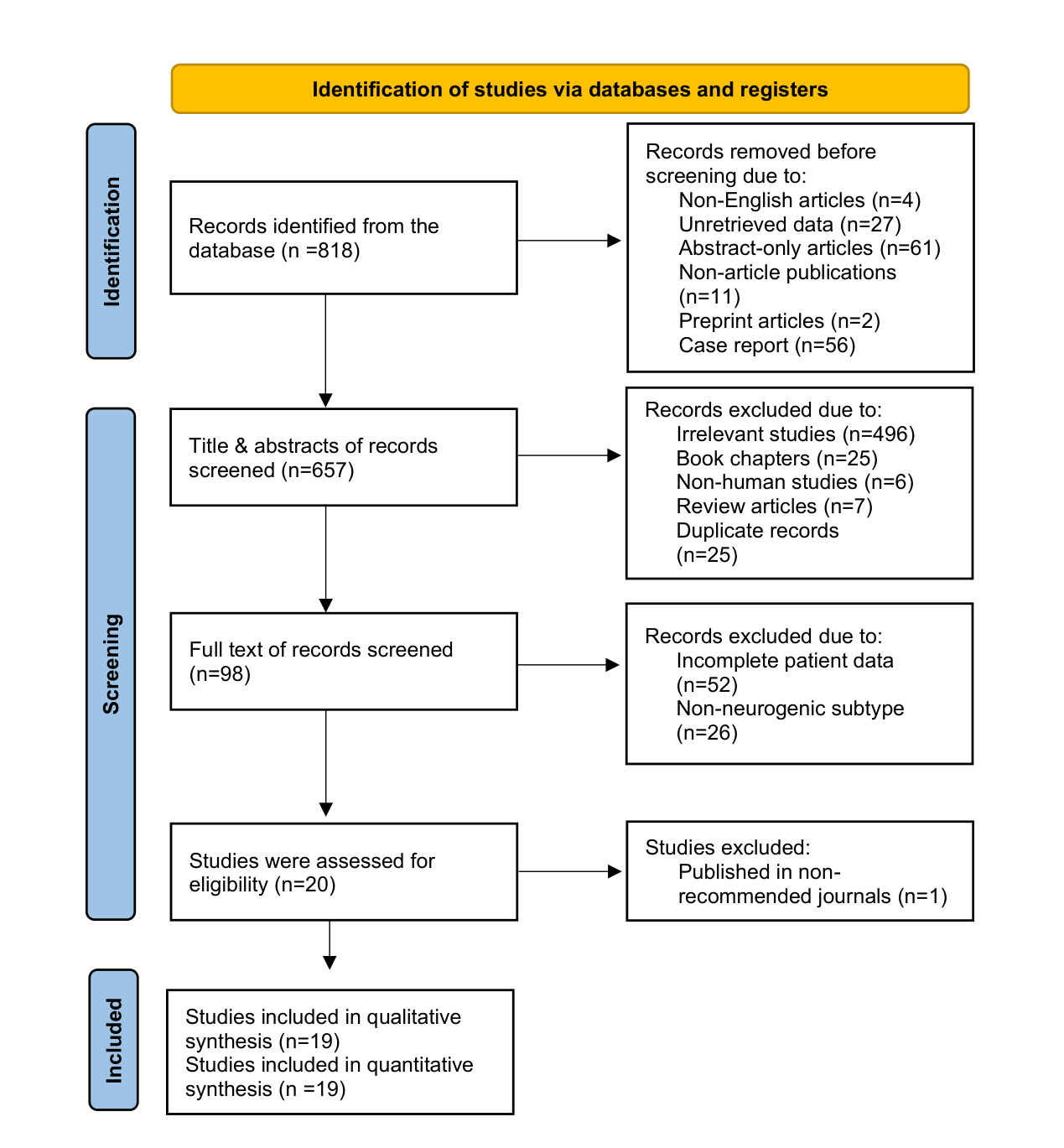
A total of 816 records were initially identified through database searching. After exclusion of non-English articles, studies with unretrieved data, abstract-only publications, non-article publications, preprints, and case reports, 657 records remained for title and abstract screening. Of these, 559 records were excluded because they consisted of irrelevant studies, book chapters, non-human studies, review articles, or duplicate records. Subsequently, 98 full-text articles were assessed for eligibility. Following full-text evaluation, studies with incomplete patient data, studies involving non-neurogenic TOS subtypes, and studies published in non-recommended journals were excluded. Ultimately, 20 studies were assessed for eligibility, of which 1 was excluded because it was published in a non-recommended journal (Figure 1). The final analysis included 19 studies [12,15,16,18–33], two of which were identified through AI-assisted tools [12,33]. Collectively, these studies involved 771 patients and 1,334 operated sides. Most included studies were cohort studies (14/19, 73.68%), followed by case series (4/19, 21.05%) and one randomized controlled trial (1/19, 5.26%). Eighteen studies (94.74%) were conducted in a single-center setting, whereas one study (5.26%) was multicenter. Among the reported sex data, females accounted for 906 cases (75.44%) and males for 295 cases (24.56); two studies did not report sex distribution. The mean age of patients across the included studies ranged from 27.8 to 44.8 years (Table 1). Preoperative conservative treatment was reported in 1,197 operated sides (89.73%), whereas 137 sides (10.27%) underwent surgery without documented prior conservative management (Table 2). Overall postoperative outcome data were available for 1,285 operated sides after exclusion of 18 patients with unavailable outcome data. Successful outcomes were observed in 1,119 cases (87.08%), whereas 166 cases (12.92%) were categorized as failures (Table 3). The success rate was 87.46% for the transaxillary approach (607/694 analyzable cases), 83.43% for the supraclavicular approach (292/350), 93.33% for video-assisted thoracoscopic surgery (VATS) (112/120), and 100.00% for robotic-assisted thoracoscopic surgery (RATS) (10/10). No statistically significant difference in success rates was identified between the transaxillary and supraclavicular approaches (P = 0.075) (Table 4). Complication-related data were available for 877 operated sides (65.74%). Among the 481 operated sides managed via the transaxillary approach with available complication data, 170 complications were recorded. Pneumothorax was the most frequently reported complication in both the transaxillary (n = 99, 20.58%) and supraclavicular (n = 7, 2.68%) approaches. Recurrence data revealed an overall recurrence rate of 1.50% (n = 20) (Table 5). The supraclavicular approach was associated with the highest absolute recurrence rate among the two principal open techniques, with 7 recurrences recorded among 363 operated sides (1.93%). The transaxillary approach yielded 11 recurrences among 724 operated sides (1.52%). Statistical comparison between the supraclavicular and transaxillary approaches demonstrated no significant difference in recurrence rates (P = 0.618) (Table 6).
|
First Author |
Year |
Country |
Study Design |
Patients with NTOS |
No. of Op. sides |
No. of Centers |
Male (n) |
Female (n) |
Mean Age (year) |
Age Range |
Unilateral |
Bilateral |
Right Side |
Left Side |
|
Derdiyok [15] |
2024 |
Turkey |
Case series |
13 |
13 |
Single |
10 |
3 |
37.23 ± 5.73 |
28–46 |
13 |
0 |
9 |
4 |
|
Dua [18] * |
2020 |
USA |
Cohort |
N/A |
102 |
Single |
24 |
78 |
29.8 |
14–64 |
N/A |
N/A |
N/A |
N/A |
|
George [19] |
2016 |
United Kingdom |
Case series |
9 |
11 |
Single |
2 |
7 |
33.11 ± 4.91 |
25–43 |
7 |
2 |
6 |
5 |
|
Kocher [20] |
2018 |
Switzerland |
Case series |
4 |
5 |
Single |
1 |
3 |
43.25 ± 20.56 |
25–43 |
3 |
1 |
3 |
2 |
|
Li [21] |
2021a |
China |
Cohort |
30 |
31 |
Single |
7 |
23 |
38.6 ± 13.14 |
N/A |
29 |
1 |
N/A |
N/A |
|
Li [21] |
2021b |
China |
Cohort |
26 |
28 |
Single |
6 |
20 |
40.38 ± 10.89 |
N/A |
24 |
2 |
N/A |
N/A |
|
Nuutinen [22] * |
2021 |
Finland |
Cohort |
20 |
27 |
Single |
6 |
21 |
41.8 ± 10.3 |
N/A |
13 |
7 |
14 |
13 |
|
Nuutinen [23] |
2022a |
Finland |
Cohort |
15 |
18 |
Single |
3 |
12 |
44.8 ± 12.5 |
N/A |
11 |
4 |
9 |
9 |
|
Nuutinen [23] |
2022b |
Finland |
Cohort |
18 |
22 |
Single |
5 |
13 |
43.4 ± 10.8 |
N/A |
14 |
4 |
11 |
11 |
|
Ochuba [24] * |
2022 |
USA |
Cohort |
208 |
243 |
Single |
54 |
189 |
35.86 ± 12.8 |
N/A |
35 |
173 |
N/A |
N/A |
|
Rochlin [25] |
2013 |
USA |
Cohort |
87 |
104 |
Single |
15 |
72 |
41 |
21–63 |
70 |
17 |
N/A |
N/A |
|
Rochlin [26] |
2014 |
USA |
Cohort |
30 |
55 |
Single |
N/A |
N/A |
N/A |
N/A |
5 |
25 |
25 |
25 |
|
Whiley [27] |
2023 |
Australia |
Case series |
19 |
23 |
Single |
10 |
9 |
29.4 ± 9.0 |
18–48 |
15 |
4 |
N/A |
N/A |
|
Azenha [16] |
2022 |
Switzerland |
Cohort |
5 |
5 |
Multi |
0 |
5 |
N/A |
N/A |
5 |
0 |
3 |
2 |
|
Chandra [28] |
2011a |
USA |
Cohort |
34 |
34 |
Single |
11 |
23 |
39 |
N/A |
34 |
0 |
N/A |
N/A |
|
Chandra [28] |
2011b |
USA |
Cohort |
21 |
21 |
Single |
8 |
13 |
27.8 |
N/A |
21 |
0 |
N/A |
N/A |
|
Farquharson [12] * |
2024 |
United Kingdom |
Cohort |
N/A |
42 |
Single |
14 |
28 |
N/A |
N/A |
N/A |
N/A |
24 |
18 |
|
Gharagozloo [29] * |
2021 |
USA |
Cohort |
79 |
79 |
Single |
29 |
50 |
34 ± 9.5 |
N/A |
79 |
0 |
N/A |
N/A |
|
Goeteyn [30] * |
2022 |
The Netherlands |
RCT |
24 |
24 |
Single |
1 |
23 |
37.7 ± 9.8 |
N/A |
N/A |
N/A |
N/A |
N/A |
|
Hosn [31] * |
2020 |
USA |
Cohort |
34 |
34 |
Single |
N/A |
N/A |
N/A |
N/A |
N/A |
N/A |
N/A |
N/A |
|
Lassner [32] * |
2023a |
Germany |
Cohort |
52 |
59 |
Single |
9 |
43 |
37 |
N/A |
45 |
7 |
N/A |
N/A |
|
Lassner [32] * |
2023b |
Germany |
Cohort |
43 |
46 |
Single |
11 |
32 |
38.1 |
N/A |
40 |
3 |
N/A |
N/A |
|
Orlando [33] * |
2015 |
USA |
Cohort |
N/A |
308 |
Single |
69 |
239 |
35.9 |
13–63 |
N/A |
N/A |
149 |
159 |
|
NTOS = neurogenic thoracic outlet syndrome; N/A = not available; Op = Operated. Studies marked with an asterisk (*) indicate that the reported total number of males and females was calculated based on the total number of operated sides rather than the total number of patients. Studies with the same first author and publication year, differentiated by suffixes (a/b), represent separate cohorts or operative groups reported from the same research group. |
||||||||||||||
|
First Author |
Year |
Conservative Treatment |
Conservative Duration |
Type of Conservative Therapy |
Pre-op BTX Injection |
Surgical Approach |
Type of Rib Resection |
Mean OP Time |
OP Time Range |
Mean Follow-up |
Follow-up Range |
|
Derdiyok [15] |
2024 |
Yes |
6 months |
Physiotherapy, medical treatment |
No |
VATS |
Complete/near-complete |
81 ± 11 min |
65–100 min |
19 ± 13 months |
2–38 months |
|
Dua [18] |
2020 |
Yes |
3–6 months |
Physiotherapy |
Yes |
Supraclavicular |
Not reported |
N/A |
N/A |
3.7 years |
1–16.9 years |
|
George [19] |
2016 |
Yes |
≥6 months |
Physiotherapy |
No |
VATS |
Complete/near-complete |
85 min a |
65–90 min |
6 months |
N/A |
|
Kocher [20] |
2018 |
Yes |
6 months |
Physiotherapy |
No |
Robotic-assisted transthoracic |
Complete/near-complete |
99.83 ± 19.12 min |
80–120 min |
3 months |
N/A |
|
Li [21] |
2021a |
Yes |
≥3 months |
Physiotherapy |
No |
Modified supraclavicular (conventional) |
Complete/near-complete |
143.33 ± 25.64 min |
N/A |
27.37 ± 27.2 months |
12–67 months |
|
Li [21] |
2021b |
Yes |
≥3 months |
Physiotherapy |
No |
Modified supraclavicular (piezo surgery) |
Complete/near-complete |
96.85 ± 14.66 min |
N/A |
21.77 ± 24.5 months |
12–60 months |
|
Nuutinen [22] |
2021 |
Yes |
≥6 months |
Manual therapy, therapeutic exercises, and pain medication |
No |
Transaxillary |
Subtotal/partial |
N/A |
N/A |
14.9 ± 3.6 years |
11–21 years |
|
Nuutinen [23] |
2022a |
Yes |
≥6 months |
Manual therapy, therapeutic exercises, and pain medication |
No |
Transaxillary |
Subtotal/partial |
N/A |
N/A |
94.5 ± 18.9 months |
N/A |
|
Nuutinen [23] |
2022b |
Yes |
≥6 months |
Manual therapy, therapeutic exercises, and pain medication |
No |
VATS |
Subtotal/partial |
N/A |
N/A |
50.4 ± 11.7 months |
N/A |
|
Ochuba [24] |
2022 |
Yes |
N/A |
Physical therapy, muscle relaxants, anti-inflammatory agents, ergonomic modifications, and scalene injections |
Yes |
Transaxillary |
Complete/near-complete |
N/A |
N/A |
44.9 months a |
N/A |
|
Rochlin [25] |
2013 |
Yes |
N/A |
Physical therapy |
Yes |
Transaxillary |
Not reported |
N/A |
N/A |
44.7 months |
12.4–91.9 months |
|
Rochlin [26] |
2014 |
Yes |
2 months |
Physical therapy |
Yes |
Transaxillary / supraclavicular |
Not reported |
N/A |
N/A |
N/A |
N/A |
|
Whiley [27] |
2023 |
Yes |
N/A |
Physiotherapy |
No |
N/A |
Not reported |
N/A |
N/A |
12 months b |
N/A |
|
Azenha [16] |
2022 |
Yes |
≥3 months |
Physical therapy, postural training, oral analgesics |
No |
RATS |
Complete/near-complete |
N/A |
N/A |
N/A |
N/A |
|
Chandra [28] |
2011a |
No |
N/A |
N/A |
No |
Supraclavicular |
Subtotal/partial |
N/A |
N/A |
1 year b |
N/A |
|
Chandra [28] |
2011b |
Yes |
≥2 months |
Edgelow protocol |
No |
Supraclavicular |
Subtotal/partial |
N/A |
N/A |
6 months to 2 years b |
N/A |
|
Farquharson [12] |
2024 |
Yes |
N/A |
Physiotherapy (95%) |
No |
Supraclavicular |
Not specified |
N/A |
N/A |
6 months b |
N/A |
|
Gharagozloo [29] |
2021 |
No |
N/A |
N/A |
No |
VATS |
Subtotal/partial |
87.6 ± 10.8 min |
N/A |
6 months b |
N/A |
|
Goeteyn [30] |
2022 |
No |
N/A |
N/A |
No |
Transaxillary |
Complete/near-complete |
N/A |
N/A |
12 months b |
N/A |
|
Hosn [31] |
2020 |
Yes |
N/A |
Physical therapy |
No |
18 transaxillary, 16 supraclavicular |
Subtotal/partial |
N/A |
N/A |
N/A |
N/A |
|
Lassner [32] |
2023a |
Yes |
N/A |
Physiotherapy, anti-inflammatory medications, and analgesics |
No |
Supraclavicular |
Complete/near-complete |
N/A |
N/A |
≥1 year c |
N/A |
|
Lassner [32] |
2023b |
Yes |
N/A |
Physiotherapy, anti-inflammatory medications, and analgesics |
No |
Supraclavicular |
Subtotal/partial |
N/A |
N/A |
≥1 year c |
N/A |
|
Orlando [33] |
2015 |
Yes |
2 months |
Physical therapy |
Yes |
Transaxillary |
Subtotal/partial |
N/A |
N/A |
N/A |
N/A |
|
a median, b follow-up duration applied equally to all patients, c minimum follow-up duration. BTX = botulinum toxin; VATS = video-assisted thoracoscopic surgery; RATS = robotic-assisted thoracoscopic surgery. N/A = not available; Edgelow protocol = structured physical therapy program for TOS. |
|||||||||||
|
First Author |
Year |
Outcome Grade (n) |
Overall outcome (n) |
Success rate (%) |
Overall Complications (n) |
Complications Detail |
Recurrence (n) |
||||||
|
Excellent |
Good |
Fair |
Poor |
N/A |
Success |
Failure |
N/A |
||||||
|
Derdiyok [15] |
2024 |
0 |
9 |
1 |
0 |
3 |
9 |
1 |
3 |
90.00% |
1 |
1 Transient neurological deficit |
0 |
|
Dua [18] * |
2020 |
N/D |
N/D |
N/D |
N/D |
N/D |
88 |
14 |
0 |
86.27% |
N/A |
N/A |
0 |
|
George [19] |
2016 |
8 |
1 |
0 |
0 |
0 |
9 |
0 |
0 |
100.00% |
2 |
1 Superficial wound infection, 1 transient neurological deficit |
0 |
|
Kocher [20] * |
2018 |
5 |
0 |
0 |
0 |
0 |
5 |
0 |
0 |
100.00% |
0 |
None |
0 |
|
Li [21] |
2021a |
13 |
9 |
4 |
4 |
0 |
22 |
8 |
0 |
73.33% |
2 |
1 lymphorrhoea, 1 hemorrhage |
0 |
|
Li [21] |
2021b |
15 |
8 |
2 |
1 |
0 |
23 |
3 |
0 |
88.46% |
0 |
None |
0 |
|
Nuutinen [22] * |
2021 |
13 |
9 |
3 |
2 |
0 |
22 |
5 |
0 |
81.48% |
0 |
None |
0 |
|
Nuutinen [23] * |
2022a |
1 |
14 |
0 |
3 |
0 |
15 |
3 |
0 |
83.33% |
2 |
1 brachial plexus injury, 1 persistent iatrogenic Horner syndrome |
0 |
|
Nuutinen [23] * |
2022b |
7 |
10 |
3 |
2 |
0 |
17 |
5 |
0 |
77.27% |
1 |
1 Numbness of the operated chest wall |
0 |
|
Ochuba [24] * |
2022 |
143 |
61 |
15 |
24 |
0 |
204 |
39 |
0 |
83.95% |
N/A |
N/A |
0 |
|
Rochlin [25] |
2013 |
N/D |
N/D |
N/D |
N/D |
N/D |
63 |
18 |
6 |
77.78% |
75 |
26 pains, 19 pneumothoraces, 18 scar tissue formations, 7 reinjuries, 5 swellings |
10 |
|
Rochlin [26] * |
2014 |
N/D |
N/D |
N/D |
N/D |
N/D |
46 |
8 |
1 |
85.19% |
17 |
11 pneumothoraces, 3 wound healing problems, 1 postoperative hematoma, 1 scapular winging, 1 avulsed branch of the subclavian artery |
2 |
|
Whiley [27] * |
2023 |
N/D |
N/D |
N/D |
N/D |
N/D |
22 |
1 |
0 |
95.65% |
N/A |
N/A |
0 |
|
Azenha [16] * |
2022 |
N/D |
N/D |
N/D |
N/D |
N/D |
5 |
0 |
0 |
100.00% |
2 |
1 pneumothorax, 1 recurrent pleural effusion |
0 |
|
Chandra [28] |
2011a |
N/D |
N/D |
N/D |
N/D |
N/D |
19 |
15 |
0 |
55.88% |
5 |
2 wound seromas requiring drainage, 3 pneumothoraces requiring tube thoracostomy |
0 |
|
Chandra [28] |
2011b |
N/D |
N/D |
N/D |
N/D |
N/D |
19 |
2 |
0 |
90.48% |
2 |
1 pneumothorax, 1 lymphocele |
0 |
|
Farquharson [12] * |
2024 |
N/D |
N/D |
7 |
2 |
0 |
33 |
9 |
0 |
78.57% |
10 |
3 pneumothoraces, 2 phrenic nerve complications, 2 hematomas, 1 brachial neuropraxia, 1 hemothorax, 1 Wound infection |
0 |
|
Gharagozloo [29] |
2021 |
N/D |
N/D |
N/D |
N/D |
N/D |
77 |
2 |
0 |
97.47% |
9 |
9 persistent paresthesia |
0 |
|
Goeteyn [30] |
2022 |
N/D |
N/D |
N/D |
N/D |
N/D |
22 |
2 |
0 |
91.67% |
5 |
2 neuropathic pains of the intercostobrachial nerve, 1 surgical site infection, 1 transient Horner syndrome, 1 transient phrenic nerve palsy |
1 |
|
Hosn [31] |
2020 |
N/D |
N/D |
N/D |
N/D |
N/D |
30 |
4 |
0 |
88.24% |
N/A |
N/A |
0 |
|
Lassner [32] |
2023a |
N/D |
N/D |
N/D |
N/D |
N/D |
50 |
2 |
0 |
96.15% |
1 |
1 transient Horner syndrome |
2 |
|
Lassner [32] |
2023b |
N/D |
N/D |
N/D |
N/D |
N/D |
38 |
5 |
0 |
88.37% |
5 |
2 transient Horner syndromes, 1 transient phrenic nerve palsy, 1 pleural injury (no drainage required), 1 long thoracic nerve palsy (transient) |
5 |
|
Orlando [33] * |
2015 |
N/D |
N/D |
N/D |
N/D |
N/D |
281 |
20 |
7 |
93.36% |
88 |
80 pneumothoraces, 4 wound infections, 2 hematomas, 1 hemothorax, 1 vein injury |
0 |
|
N/D = not distinguishable (outcome subcategories were not reported separately and could not be converted). N/A = not available/not reported. Studies marked with an asterisk (*) indicate that the reported total overall results and outcome grade were calculated based on the total number of operated sides rather than the total number of patients. Outcome grading (where reported): Excellent / Good = successful; Fair / Poor = Failure. |
|||||||||||||
|
Variable |
Total (n) a |
Analyzable Cases (Excl. N/A) (n) |
Overall outcome |
Success Rate (%) |
P-value e |
||
|
Success (n) |
Failure (n) |
N/A (n) |
|||||
|
Surgical Approach b,c |
|||||||
|
Transaxillary |
707 |
694 |
607 |
87 |
13 |
87.46% |
0.075 |
|
Supraclavicular |
350 |
350 |
292 |
58 |
0 |
83.43% |
|
|
VATS |
123 |
120 |
112 |
8 |
3 |
93.33% |
— |
|
RATS |
10 |
10 |
10 |
0 |
0 |
100.00% |
|
|
Extent of Resection d |
|||||||
|
Complete/Near-complete resection |
407 |
404 |
349 |
55 |
3 |
86.39% |
0.141 |
|
Subtotal/Partial resection |
586 |
579 |
518 |
61 |
7 |
89.46% |
|
|
BTX injection |
|||||||
|
Yes |
795 |
781 |
682 |
99 |
14 |
87.32% |
0.747 |
|
No |
507 |
504 |
437 |
67 |
3 |
86.71% |
|
|
N/A = not available; n = number; RATS = robot-assisted thoracoscopic surgery; VATS = video-assisted thoracoscopic surgery; Excl. = excluding; BTX = botulinum toxin a Reported totals were calculated according to the data presentation of each included study. Some studies reported outcomes based on the total number of patients, whereas others reported outcomes according to the total number of operated sides. Accordingly, the pooled totals represent the combined number of patients and operated sides, as originally reported. b Studies that included two surgical approaches without separately distinguishing outcomes for each group were excluded from this analysis. c Studies in which the surgical approach was not reported were also excluded from this table. d Studies that did not clearly distinguish the extent of resection were excluded from this analysis. e P-value calculated using the Pearson Chi-square test comparing success and failure rates. |
|||||||
|
Total Number of Patients a |
771 patients |
|
Total number of operated sides |
1,334 sides |
|
Study design |
n = 19, (%) |
|
Cohort |
14 (73.68%) |
|
Case series |
4 (21.05%) |
|
RCT |
1 (5.26%) |
|
Study setting |
n = 19, (%) |
|
Single-center study |
18 (94.74%) |
|
Multicenter study |
1 (5.26%) |
|
Country of the corresponding author |
n = 19, (%) |
|
USA |
8 (42.11%) |
|
Finland |
2 (10.53%) |
|
Switzerland |
2 (10.53%) |
|
United Kingdom |
2 (10.53%) |
|
Australia |
1 (5.26%) |
|
China |
1 (5.26%) |
|
Germany |
1 (5.26%) |
|
The Netherlands |
1 (5.26%) |
|
Türkiye |
1 (5.26%) |
|
Sex b,c |
n = 1,201, (%) |
|
Female |
906 (75.44%) |
|
Male |
295 (24.56%) |
|
Laterality b |
n = 1,218, (%) |
|
Unilateral |
458 (37.60%) |
|
Bilateral |
250 (20.53%) |
|
N/A |
510 (41.87%) (5 studies) |
|
Preoperative conservative treatment |
n = 1,334, (%) |
|
Yes |
1197 (89.73%) |
|
No |
137 (10.27%) |
|
Conservative treatment duration |
n = 1,334, (%) |
|
At least 2 months |
384 (28.79%) |
|
At least 3 months |
166 (12.44%) |
|
At least 6 months |
96 (7.19%) |
|
N/A |
688 (51.57%) |
|
Complications d |
n = 877, (%) |
|
Transaxillary approach |
n = 481, (%) |
|
Pneumothorax |
99 (20.58%) |
|
Pain |
26 (5.40%) |
|
Scar tissue formation |
18 (3.74%) |
|
Reinjury |
7 (1.45%) |
|
Infection |
5 (1.04%) |
|
Swelling |
5 (1.04%) |
|
Neuropathic pain |
2 (0.42%) |
|
Hematoma |
2 (0.42%) |
|
Horner syndrome |
2 (0.42%) |
|
Brachial plexus injury |
1 (0.21%) |
|
Phrenic nerve palsy |
1 (0.21%) |
|
Hemothorax |
1 (0.21%) |
|
Vein injury |
1 (0.21%) |
|
No complication |
311 (64.66%) |
|
Supraclavicular approach |
n = 261, (%) |
|
Pneumothorax |
7 (2.68%) |
|
Horner syndrome |
3 (1.15%) |
|
Phrenic nerve palsy |
3 (1.15%) |
|
Hematoma / Hemorrhage |
3 (1.15%) |
|
Lymphatic complication |
2 (0.77%) |
|
Wound seroma |
2 (0.77%) |
|
Brachial neuropraxia |
1 (0.38%) |
|
Hemothorax |
1 (0.38%) |
|
Wound infection |
1 (0.38%) |
|
Pleural injury |
1 (0.38%) |
|
Long thoracic nerve palsy |
1 (0.38%) |
|
No complication |
236 (90.42%) |
|
VATS |
n = 125, (%) |
|
Paresthesia / Numbness |
10 (8.00%) |
|
Transient neurological deficit |
2 (1.60%) |
|
Superficial wound infection |
1 (0.80%) |
|
No complication |
112 (89.60%) |
|
No complication |
112 (89.60%) |
|
RTAS |
n = 10, (%) |
|
Pneumothorax |
1 (10.00%) |
|
Recurrent pleural effusion |
1 (10.00%) |
|
No complication |
8 (80.00%) |
|
N/A |
457 (34.26%) |
|
Overall outcome b, e |
n = 1,285, (%) |
|
Success |
1119 (87.08%) |
|
Failure |
166 (12.92%) |
|
Overall recurrence f |
n = 1,334, (%) |
|
No |
1,314 (98.50%) |
|
Yes |
20 (1.50%) |
|
RCT = randomized controlled trial; USA = united states of America; BTX = botulinum toxin; VATS = video-assisted thoracoscopic surgery; RATS = robotic-assisted thoracic surgery a The study by Dua et al., Farquharson et al, and Orlando et al. did not report the total number of patients in their study; they reported the total number of operated sides. b Some studies reported data based on the total number of operated sides, while others reported data based on the total number of individual patients; therefore, the totals may not correspond to the overall number of patients included. c Two studies did report the sex distribution (n = 89) d Four studies (Dua et al., Ochuba et al., Whiley et al., Azenha et al., and Hosn et al.) did not report complication-related data. e Eighteen patients with unavailable outcome data were excluded from the analysis. f Studies that did not report recurrence were considered to have zero recurrence events. |
|
|
Variable |
Total Operated Sides, n a |
Recurrent, n b |
Recurrence Rate, % |
P-value c |
|
Surgical Approach |
||||
|
Supraclavicular |
363 |
7 |
1.93% |
0.618 |
|
Transaxillary |
724 |
11 |
1.52% |
|
|
RATS |
10 |
0 |
0.00% |
— |
|
VATS |
125 |
0 |
0.00% |
— |
|
Extent of Resection |
||||
|
Complete/Near-complete resection |
419 |
3 |
0.72% |
0.815 |
|
Subtotal/Partial resection |
589 |
5 |
0.85% |
|
|
RATS = robot-assisted thoracoscopic surgery; VATS = video-assisted thoracoscopic surgery a The totals were calculated based on the total number of operated sides rather than the total number of patients. b Studies that did not report recurrence were considered to have zero recurrence events. c P-value was calculated using the Pearson Chi-square test. |
||||
Discussion
Neurogenic TOS predominantly affects young to middle-aged adults during the active working years of life, with a well-documented female predominance consistently reported across clinical series. Females constitute approximately 70% of the TOS surgical population and may possess predisposing anatomical and mechanical factors that contribute to the higher prevalence observed across TOS subtypes [34]. In the present review, females accounted for 75.44% of patients with available sex data, closely aligning with the approximately 70% prevalence previously reported, thereby supporting the representativeness of the included study population within the broader nTOS surgical cohort. The mean age across the included studies ranged from 27.8 to 44.8 years, corroborating the established pattern of NTOS presentation in the third to fifth decades of life and underscoring the significant functional and socioeconomic burden of this condition, given its predilection for active working-age individuals.
The efficacy of FRR for NTOS has been evaluated across a range of operative approaches and patient populations, and the evidence consistently supports a clinically meaningful symptomatic benefit for the majority of patients who undergo surgical decompression. In a systematic review and meta-analysis by Blondin et al. comparing patient-reported functional outcomes across surgical approaches for NTOS, the transaxillary approach yielded a Derkash-based success rate of 87.9%, and the supraclavicular approach 93.2% [35]. The treatment of NTOS has historically been hampered by inconsistent definitions, variable diagnostic criteria, and the absence of standardized outcome measures, all of which contribute to the wide variation in reported success rates across series [1]. In this review, an overall success rate of 87.08% was observed across 1,285 analyzable operated sides, consistent with the range reported in the contemporary literature.
The choice of operative approach for FRR in NTOS has been the subject of sustained debate. Both the transaxillary and supraclavicular approaches are widely used and considered effective, with each offering distinct advantages in operative exposure, the extent of rib resection achievable, and the capacity to perform adjunctive procedures [31]. Comparative institutional series have consistently shown similar decompression and symptom-resolution rates between the two approaches, with no significant differences in overall outcomes [31]. The Blondin et al. meta-analysis further demonstrated that, although numerical differences in success rates existed between approaches, both transaxillary and supraclavicular FRR achieved clinically meaningful improvement in the majority of patients [35]. Consistent with this evidence, the present review found that the success rate for the transaxillary approach (87.46%) did not differ significantly from that of the supraclavicular approach (83.43%; P = 0.075), supporting the view that surgeon expertise and patient-specific anatomical considerations, rather than the approach per se, are the principal determinants of outcome.
Minimally invasive techniques for FRR, including VATS and RATS, have emerged as increasingly viable alternatives to conventional open approaches. A systematic review of robotic FRR by Reyes et al., encompassing 12 studies and 397 patients across all TOS subtypes, demonstrated that robotic FRR is associated with favorable intraoperative outcomes, including minimal blood loss and low conversion rates to open approaches, and that patients experience decreased pain, improved function, and low postoperative complication rates [36]. Nuutinen et al., in a direct long-term comparison of transaxillary versus VATS-based FRR for NTOS, found no significant differences in long-term outcomes between the two techniques, with both approaches offering favorable results at a mean follow-up of approximately six years [23]. In the present study, the success rate for VATS was 93.33% across 120 analyzable sides, and the success rate for RATS was 100% across 10 sides, both numerically exceeding those of the conventional open techniques. Neither the VATS nor the RATS cohorts recorded any recurrences, further supporting the potential durability of minimally invasive decompression, though the limited sample sizes, particularly for RATS, preclude formal statistical comparisons and require validation in larger prospective series.
The extent of FRR has been proposed as a determinant of both immediate surgical success and long-term durability. Likes et al. demonstrated that patients presenting with recurrent NTOS symptoms attributable to a residual first rib uniformly improved following re-resection, providing direct clinical evidence for the pathogenic role of incomplete bony decompression and establishing the residual rib as the primary cause of recurrent TOS in their series [37]. Lassner et al., in a retrospective study comparing costovertebral exarticulation with conventional resection, reported significantly better outcomes in the exarticulation group (P < 0.001), supporting the hypothesis that the proximal portion of the first rib plays a pivotal role in the pathogenesis of NTOS in a subset of patients [32]. Conversely, a recent randomized controlled trial comparing conventional first-rib resection with first-rib avulsion found no statistically significant differences in postoperative pain relief, numbness reduction, or patient satisfaction between the two techniques, despite significantly longer rib removal in the avulsion group, suggesting that greater rib excision may not necessarily translate into superior short-term clinical outcomes [38]. In this study, however, no statistically significant difference in success rate was identified between complete or near-complete resection (86.39%) and subtotal or partial resection (89.46%; P = 0.141), nor between these groups in terms of recurrence (0.72% versus 0.85%; P = 0.815). These findings may reflect inconsistent definitions of resection completeness across the included studies and the relatively short follow-up durations, which may be insufficient to capture late recurrences attributable to residual rib-stimulated fibrosis. Prospective studies with standardized definitions of resection extent and long-term follow-up are required to resolve this issue definitively.
Surgical decompression for NTOS carries a well-characterized spectrum of postoperative complications, the nature and frequency of which vary substantially according to the operative approach employed. Blondin et al. documented complication rates of 14.5% and 8.7% for the transaxillary and supraclavicular approaches, respectively, in their meta-analysis, with pneumothorax representing the predominant complication of transaxillary FRR [35]. In the present review, pneumothorax was the most frequently documented complication in the transaxillary cohort, occurring in 20.58% of operated sides with available complication data, a figure consistent with published estimates and reflecting the inherent proximity of the pleural surface to the operative field in this approach.
In contrast to the transaxillary approach, the supraclavicular technique is associated with a distinct complication profile related to the cervical dissection plane. Lassner et al. documented approach-specific complications of the supraclavicular route in their institutional series, including transient Horner syndrome, phrenic nerve palsy, and pleural injury, reflecting the recognized anatomical hazards of dissection in the supraclavicular field [32]. In the present review, the supraclavicular cohort demonstrated a substantially lower pneumothorax rate (2.68%), with Horner syndrome (1.15%), phrenic nerve palsy (1.15%), and lymphatic complications (0.77%) constituting the predominant approach-specific adverse events, consistent with the complication profiles reported by Lassner et al. [32]. Standardization of complication reporting using validated classification frameworks remains an unmet need in the NTOS surgical literature; four studies in this review did not report complication data at all, introducing a potential underestimation bias in the pooled estimates of complications [18,24,27,31].
The complication profile of minimally invasive FRR differs from that of conventional open approaches, and this has been proposed as one of the principal advantages of the thoracoscopic perspective. Reyes et al. noted that the improved exposure afforded by robotic FRR reduces the risk of injury to neurovascular structures and is associated with shorter hospital stays compared with traditional approaches [36]. In this study, the VATS cohort demonstrated a complication profile characterized predominantly by paresthesia and numbness (8.00%) and transient neurological deficits (1.60%), without clinically significant pleural complications requiring drainage. In contrast, the RATS cohort recorded complications in 2 of 10 operated sides (20.00%), comprising one case of pneumothorax (10.00%) and one case of recurrent pleural effusion (10.00%); both represent pleural complications likely attributable to the intrathoracic nature of the robotic operative approach rather than indicative of major neurovascular morbidity. These figures should be interpreted with caution, given the small sample size, and are not inconsistent with the broader robotic FRR literature, in which pleural complications have been reported at low but non-negligible rates [16,36]. As experience with thoracoscopic FRR matures and robotic platforms become more widely accessible, these minimally invasive approaches may assume a more prominent role in the NTOS management algorithm.
Recurrence following FRR for NTOS is a recognized clinical challenge with well-characterized mechanisms. Roos described a cohort of 76 patients who required reoperation for disabling recurrent TOS following initial transaxillary FRR, observing that a subset of patients gradually developed recurrent neurological symptoms attributable to postoperative scar tissue entrapping segments of the brachial plexus, and that two distinct patterns of recurrence were identifiable, both capable of progressing to a state refractory to all conservative measures [39]. Likes et al. subsequently confirmed that retained bony remnants are a principal driver of recurrence, demonstrating that all 15 patients in their series who underwent re-resection of a remaining or residual first rib achieved clinical improvement in the postoperative period, supporting the practice of complete rib removal at the index procedure to prevent recurrence [37]. In the current dataset, the supraclavicular approach was associated with a marginally higher absolute recurrence rate (1.93%) compared with the transaxillary approach (1.52%), a difference that did not reach statistical significance (P = 0.618). The notably low overall recurrence rate of 1.50% observed is consistent with these findings, though it must be interpreted with caution, given the relatively short follow-up periods in most included studies, as recurrence following FRR may not manifest within such short observation periods.
This systematic review is subject to several limitations that should be considered when interpreting its findings. First, there was substantial heterogeneity in postoperative outcome reporting across the included studies. The absence of a universally accepted and validated outcome measure for NTOS required the use of a standardized binary and ordinal outcome classification framework. Although this approach improved cross-study comparability, it introduced a degree of subjectivity when heterogeneous outcome descriptions were mapped into unified categories, potentially resulting in loss of detail from the original reports. Second, most included studies were retrospective cohort studies or case series, with only one randomized controlled trial identified. Retrospective designs are inherently prone to selection bias, information bias, and incomplete follow-up, thereby limiting the overall quality of evidence. In addition, the predominance of single-center studies restricts the generalizability of the pooled findings. Third, incomplete and inconsistent reporting was common across the included literature. Several studies did not provide complication data, exact follow-up durations, or complete demographic characteristics. Studies without reported recurrence data were considered to have zero recurrence events, which may have underestimated the true recurrence rate. Similarly, incomplete complication reporting may have led to underestimation of the actual postoperative complication burden. Fourth, follow-up durations were highly variable and frequently short. Because recurrence following FRR may occur gradually over years due to scar tissue formation or brachial plexus re-entrapment, limited follow-up periods may underestimate the true long-term recurrence rate. Consequently, the low recurrence rate observed in this review should be interpreted cautiously. Fifth, minimally invasive approaches were underrepresented. The relatively small numbers of VATS and robotic-assisted procedures limited the ability to perform reliable statistical comparisons with conventional open techniques and restricted conclusions regarding their relative efficacy and safety. Sixth, the literature search was primarily conducted through Google Scholar using the allintitle feature and supplemented with AI-assisted search tools. Although this strategy was designed to improve retrieval efficiency, the absence of comprehensive multi-database searching may have resulted in the omission of relevant studies. Furthermore, this review was not prospectively registered before data collection, which limits methodological transparency. The supplementary use of AI-assisted literature retrieval is also not yet a standardized component of systematic review methodology. Finally, publication bias remains a potential concern. Studies demonstrating favorable surgical outcomes are more likely to be published than those reporting neutral or unfavorable results, which may have contributed to the overestimation of the overall success rate reported in this review.
Conclusion
First rib resection is a safe and effective treatment option for NTOS, providing favorable postoperative outcomes and low recurrence rates across various surgical approaches. Surgical success does not appear to be significantly affected by either the operative approach used or the extent of rib resection.
Declarations
Conflicts of interest: The authors have no conflicts of interest to disclose.
Ethical approval: Not applicable, as systematic reviews do not require ethical approval.
Patient consent (participation and publication): Not applicable.
Funding: The present study received no financial support.
Acknowledgments: None to be declared.
Authors' contributions: FHK contributed to Conceptualization, Methodology, Supervision, Validation, Writing – original draft, and Writing – review & editing. SKA contributed to Data curation, Formal analysis, Investigation, and Writing – review & editing. SOK contributed to Data curation, Investigation, and Writing – review & editing. AKG contributed to Methodology, Data curation, and Writing – review & editing. HSN contributed to Formal analysis, Validation, and Writing – review & editing. HAN contributed to Investigation, Methodology, Writing – original draft, and Writing – review & editing. LAS contributed to Data curation, Investigation, and Writing – review & editing. CSO contributed to Validation, Visualization, and Writing – review & editing. ASH contributed to Investigation, Methodology, and Writing – review & editing. SSM contributed to Investigation, Data curation, and Writing – review & editing. LJM contributed to Validation and Writing – review & editing. OMH contributed to Data curation and Writing – review & editing. HHA contributed to the investigation, Literature search, and writing – review & editing. HAA contributed to Data curation, Validation, and writing – review & editing. All authors read and approved the final version of the manuscript.
Use of AI: Artificial intelligence (AI) tools were used in this study for supplementary literature identification and language refinement. AI-assisted search platforms, including Consensus AI (consensus.app), Claude (Anthropic), and Perplexity AI (perplexity.ai), were used to identify potentially relevant studies in addition to the primary Google Scholar search. All records identified through these tools were screened using the same eligibility criteria applied to all retrieved studies. ChatGPT (OpenAI) was used solely for language refinement, including improvements in grammar, clarity, and readability. The authors were responsible for all aspects of the study design, study selection, data extraction, analysis, interpretation, and final manuscript content.
Data availability statement: The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
- Illig KA, Donahue D, Duncan A, Freischlag J, Gelabert H, Johansen K, et al. Reporting standards of the Society for Vascular Surgery for thoracic outlet syndrome. Journal of Vascular Surgery. 2016;64(3):e23–35. doi:10.1016/j.jvs.2016.04.039
- Kakamad F, Ghafour A, Nasralla H, Asaad S, Sabr N, Tahir S, et al. Rare etiologies of thoracic outlet syndrome: A systematic review. World Acad Sci J. 2025;7(5):1–10. doi:10.3892/wasj.2025.383
- Hooper TL, Denton J, McGalliard MK, Brismée JM, Sizer Jr PS. Thoracic outlet syndrome: a controversial clinical condition. Part 2: non-surgical and surgical management. Journal of Manual & Manipulative Therapy. 2010;18(3):132–8. doi:10.1179/106698110X12640740712338
- Moore R, Lum YW. Venous thoracic outlet syndrome. Vasc Med. 2015;20(2):182–9. doi:10.1177/1358863X14568704
- Kakamad FH, Hattam AS, Asaad SK, Ghafour AK, Raoof SS, Sharif LA, et al. Publication Trends in Thoracic Outlet Syndrome: A Bibliometric Analysis. Annals of Vascular Surgery. 2026;128:155–64. doi:10.1016/j.avsg.2026.02.055
- Jones MR, Prabhakar A, Viswanath O, Urits I, Green JB, Kendrick JB, et al. Thoracic Outlet Syndrome: A Comprehensive Review of Pathophysiology, Diagnosis, and Treatment. Pain Ther. 2019 ;8(1):5–18. doi:10.1007/s40122-019-0124-2
- Illig KA, Rodriguez-Zoppi E, Bland T, Muftah M, Jospitre E. The Incidence of Thoracic Outlet Syndrome. Annals of Vascular Surgery. 2021;70:263–72. doi:10.1016/j.avsg.2020.07.029
- Dengler NF, Pedro MT, Kretschmer T, Heinen C, Rosahl SK, Antoniadis G. Neurogenic Thoracic Outlet Syndrome—Presentation, Diagnosis, and Treatment. Dtsch Arztebl Int. 2022;119(43):735–42. doi:10.3238/arztebl.m2022.0296
- Kakamad FH, Asaad SK, Namiq HS, Ghafour AK, Hattam AS, Arif SO, et al. Current Perspectives on Pectoralis Minor Syndrome: A Narrative Review. Annals of Vascular Surgery. 2026;127:58–73. doi:10.1016/j.avsg.2026.01.037
- Fahmi H. Kakamad, Saywan K. Asaad, Abdullah K. Ghafour, Nsren S. Sabr, Hiwa S. Namiq, Lawen J. Mustafa, et al. Differential Diagnosis of Neurogenic Thoracic Outlet Syndrome: A Review. Barw Medical Journal. 2025;3(2). doi:10.58742/bmj.v3i2.161
- Fahmi H. Kakamad, Berun A. Abdalla, Saywan K. Asaad, Hawkar A. Nasralla, Abdullah K. Ghafour, Hiwa S. Namiq, et al. Provocative Tests in Diagnosis of Thoracic Outlet Syndrome: A Narrative Review. Judi Clin J. 2025;1(1):46–50. doi:10.70955/JCJ.2025.5
- Farquharson Bjm, Collis J, Jaskani S, Bergman H, Andrews B. 17 years’ experience of surgical management of thoracic outlet syndrome at a district general hospital. annals. 2024;106(1):51–6. doi:10.1308/rcsann.2023.0002
- Luu D, Seto R, Deoraj K. Exercise rehabilitation for neurogenic thoracic outlet syndrome: a scoping review. J Can Chiropr Assoc. 2022;66(1):43–60. doi:N/A
- Woodworth TT, Le A, Miller C, Conger A, Mahan MA, Cushman DM. Botulinum toxin injections for the treatment of neurogenic thoracic outlet syndrome: A systematic review. Muscle and Nerve. 2024 Jul;70(1):28–35. doi:10.1002/mus.28080
- Derdiyok O, Temel U. Videothoracoscopic First Rib Resection for Neurogenic Thoracic Outlet Syndrome: Results of 13 Patients. ATCS. 2024;30(1):n/a. doi:10.5761/atcs.oa.23-00110
- Azenha LF, Kocher GJ, Kestenholz PB, Gioutsos K, Minervini F. Thoracic outlet syndrome: a retrospective analysis of robotic assisted first rib resections. J Robotic Surg. 2022;17(3):891–6. doi:10.1007/s11701-022-01486-7
- Hiwa O. Abdullah, Berun A. Abdalla, Fahmi H. Kakamad, Jafaar O. Ahmed, Hiwa O. Baba, Marwan N. Hassan, et al. Predatory Publishing Lists: A Review on the Ongoing Battle Against Fraudulent Actions. Barw Medical Journal. 2024;2(3):26-30. doi:10.58742/bmj.v2i2.91
- Dua A, Deslarzes-Dubuis C, Rothenberg KA, Gologorsky R, Lee JT. Long-term Functional Outcomes Follow-up after 188 Rib Resections in Patients with TOS. Annals of Vascular Surgery. 2020;68:28–33. doi:10.1016/j.avsg.2020.04.033
- George RS, Milton R, Chaudhuri N, Kefaloyannis E, Papagiannopoulos K. Totally Endoscopic (VATS) First Rib Resection for Thoracic Outlet Syndrome. The Annals of Thoracic Surgery. 2017;103(1):241–5. doi:10.1016/j.athoracsur.2016.06.075
- Kocher GJ, Zehnder A, Lutz JA, Schmidli J, Schmid RA. First Rib Resection for Thoracic Outlet Syndrome: The Robotic Approach. World j surg. 2018;42(10):3250–5. doi:10.1007/s00268-018-4636-4
- Li Y, Liu Y, Zhang Z, Gao X, Cui S. A Novel Approach to First-Rib Resection in Neurogenic Thoracic Outlet Syndrome. Front Surg. 2021;8:775403. doi:10.3389/fsurg.2021.775403
- Nuutinen H, Kärkkäinen JM, Mäkinen K, Aittola V, Saari P, Pesonen J. Long-term outcome over a decade after first rib resection for neurogenic thoracic outlet syndrome. Interactive CardioVascular and Thoracic Surgery. 2021;33(5):734–40. doi:10.1093/icvts/ivab172
- Nuutinen H, Kärkkäinen JM, Kimmo M, Voitto A, Teemu R, Petri S, et al. Long-term outcomes of transaxillary versus video-assisted first rib resection for neurogenic thoracic outlet syndrome. Interactive CardioVascular and Thoracic Surgery. 2022;35(1):ivac040. doi:10.1093/icvts/ivac040
- Ochuba AJ, Mallela DP, Feghali J, Lubelski D, Belzberg AJ, Hicks CW, et al. Development and validation of a prediction model for outcomes after transaxillary first rib resection for neurogenic thoracic outlet syndrome following strict Society for Vascular Surgery diagnostic criteria. Journal of Vascular Surgery. 2023;77(2):606–15. doi:10.1016/j.jvs.2022.10.014
- Rochlin DH, Gilson MM, Likes KC, Graf E, Ford N, Christo PJ, et al. Quality-of-life scores in neurogenic thoracic outlet syndrome patients undergoing first rib resection and scalenectomy. Journal of Vascular Surgery. 2013;57(2):436–43. doi:10.1016/j.jvs.2012.08.112
- Rochlin DH, Orlando MS, Likes KC, Jacobs C, Freischlag JA. Bilateral first rib resection and scalenectomy is effective for treatment of thoracic outlet syndrome. Journal of Vascular Surgery. 2014;60(1):185–90. doi:10.1016/j.jvs.2014.01.034
- Whiley PJ, Tamhane R, Hardman DTA. A case series of first rib resection patients assessed with a novel MRI protocol for neurogenic thoracic outlet syndrome. Journal of Surgical Case Reports. 2023;2023(12):rjad672. doi:10.1093/jscr/rjad672
- Chandra V, Olcott C, Lee JT. Early results of a highly selective algorithm for surgery on patients with neurogenic thoracic outlet syndrome. Journal of Vascular Surgery. 2011;54(6):1698–705. doi:10.1016/j.jvs.2011.05.105
- Gharagozloo F, Atiquzzaman N, Meyer M, Tempesta B, Werden S. Robotic first rib resection for thoracic outlet syndrome. J Thorac Dis. 2021;13(10):6141–54. doi:10.21037/jtd-2019-rts-04
- Goeteyn J, Pesser N, Houterman S, Van Sambeek MRHM, Van Nuenen BFL, Teijink JAW. Surgery Versus Continued Conservative Treatment for Neurogenic Thoracic Outlet Syndrome: the First Randomised Clinical Trial (STOPNTOS Trial). European Journal of Vascular and Endovascular Surgery. 2022;64(1):119–27. doi:10.1016/j.ejvs.2022.05.003
- Aboul Hosn M, Goffredo P, Man J, Nicholson R, Kresowik T, Sharafuddin M, et al. Supraclavicular Versus Transaxillary First Rib Resection for Thoracic Outlet Syndrome. Journal of Laparoendoscopic & Advanced Surgical Techniques. 2020;30(7):737–41. doi:10.1089/lap.2019.0722
- Lassner F, Becker M, Prescher A. Relevance of Costovertebral Exarticulation of the First Rib in Neurogenic Thoracic Outlet Syndrome: A Retrospective Clinical Study. JPM. 2023;13(1):144. doi:10.3390/jpm13010144
- Orlando MS, Likes KC, Mirza S, Cao Y, Cohen A, Lum YW, et al. A Decade of Excellent Outcomes after Surgical Intervention in 538 Patients with Thoracic Outlet Syndrome. Journal of the American College of Surgeons. 2015;220(5):934–9. doi:10.1016/j.jamcollsurg.2014.12.046
- Cralle LE, Harris LM, Lum YW, Deery SE, Humphries MD. Thoracic outlet syndrome in females: A systematic review. Seminars in Vascular Surgery. 2023;36(4):487–91. doi:10.1053/j.semvascsurg.2023.09.003
- Blondin M, Garner GL, Hones KM, Nichols DS, Cox EA, Chim H. Considerations for Surgical Treatment of Neurogenic Thoracic Outlet Syndrome: A Meta-Analysis of Patient-Reported Outcomes. The Journal of Hand Surgery. 2023;48(6):585–94. doi:10.1016/j.jhsa.2023.03.005
- Reyes M, Alaparthi S, Roedl JB, Moreta MC, Evans NR, Grenda T, et al. Robotic First Rib Resection in Thoracic Outlet Syndrome: A Systematic Review of Current Literature. JCM. 2023;12(20):6689. doi:10.3390/jcm12206689
- Likes K, Dapash T, Rochlin DH, Freischlag JA. Remaining or Residual First Ribs Are the Cause of Recurrent Thoracic Outlet Syndrome. Annals of Vascular Surgery. 2014;28(4):939–45. doi:10.1016/j.avsg.2013.12.010
- Kakamad FH. To resect or avulse first rib in management of neurogenic thoracic outlet syndrome: a randomized controlled trial. Updates Surg. 2025;77(3):947–52. doi:10.1007/s13304-025-02125-0
- Roos DB. Recurrent thoracic outlet syndrome after first rib resection. Acta Chir Belg. 1980;79(5):363–72. doi:N/A

This work is licensed under a Creative Commons Attribution 4.0 International License.