
Epithelial-Myoepithelial Carcinoma of Salivary Glands: A Tertiary Center Experience

Abstract
Introduction
Epithelial-myoepithelial carcinoma (EMC) is a rare, biphasic malignant tumor affecting the salivary glands. It represents less than 1% of all salivary gland tumors. This study aims to present a single-center experience regarding the diagnosis, management, and prognosis of EMC.
Methods
This study was conducted between February 2020 and December 2025. Patients with a histopathologically confirmed diagnosis of epithelial-myoepithelial carcinoma were identified. Complete medical records containing demographics, clinical presentation, imaging results, histological features, treatment approaches, and follow-up results were included in the cases.
Results
Five patients were identified, of which 4 (80%) were females. The mean age was 56 ± 9.38 years. Two patients (40%) presented with painless post-auricular swelling, 1 (20%) with submandibular swelling, and 2 (40%) were incidental findings. Histopathological examination confirmed EMC in all cases. Free margins were achieved in 3 tumors (60%). No recurrence was observed during a mean follow-up of 24 ± 28.92 months.
Conclusion
Epithelial-myoepithelial carcinoma is a very rare tumor. It requires histopathological evaluation for accurate diagnosis, and complete surgical excision offers favorable short-term outcomes. Further studies are needed to better define its clinical characteristics and outcomes.
Introduction
Epithelial-myoepithelial carcinoma (EMC) is a rare, low-grade malignant neoplasm of the salivary glands characterized by its distinctive biphasic histological architecture [1-3]. It is composed of variable proportions of two cellular components arranged in double-layered duct-like structures: an inner layer of duct-lining epithelial cells and an outer layer of clear myoepithelial cells [1,2,4]. The clear myoepithelial component may predominate, occasionally complicating histopathologic interpretation [1,4].
The inner epithelial cells typically resemble intercalated duct cells and demonstrate eosinophilic cytoplasm, whereas the outer clear cells exhibit morphologic and immunophenotypic features consistent with myoepithelial differentiation [4,5]. The relative proportion of these two components may vary between tumors and within different areas of the same lesion, contributing to architectural heterogeneity [2,6].
In 1972, EMC was first described in the literature as a carcinoma [2]. However, due to its cytologic appearance, low mitotic activity, and limited nuclear pleomorphism, it was historically misclassified as a benign lesion [1,2]. It was not until 1991 that the World Health Organization (WHO) formally recognized EMC as a distinct malignant entity and classified it as a subtype of salivary gland adenocarcinoma [1,2,4].
Epithelial-myoepithelial carcinoma accounts for less than 1% of all salivary gland tumors [1]. Histologically, EMC may demonstrate multinodular growth, incomplete encapsulation, and focal infiltration into surrounding salivary gland parenchyma [2,4,6]. Despite its classification as a low-grade carcinoma, features such as perineural invasion, vascular invasion, and, in rare instances, dedifferentiation have been documented, reinforcing its malignant character [1,2,6].
The current report presents a single-center experience regarding the diagnosis, management, and prognosis of EMC. Using the most current evaluation criteria, the references were assessed for credibility [7].
Methods
Study design and setting
This single-center case series was conducted at a head and neck clinic in Iraq. The patients were managed between February 2020 and December 2025.
Inclusion and exclusion criteria
The study included patients with a confirmed histopathological diagnosis of EMC, while those with incomplete data were excluded.
Data Collection
Data were collected from the hospital’s registry and radiological reports, including demographic details, clinical presentation, medical history, histopathological reports, surgical procedures, and follow-up data.
Intervention
All cases underwent surgical intervention for parotid gland pathology via a modified lazy-S incision. Depending on the extent and characteristics of the lesion, either superficial parotidectomy or total conservative parotidectomy was performed. The procedure involved meticulous identification and preservation of the greater auricular nerve where feasible, followed by careful dissection and exploration of the facial nerve trunk and its branches to ensure nerve integrity. After complete excision of the lesion, thorough hemostasis was achieved. A surgical drain was inserted, and the wound was closed in anatomical layers.
Histopathological analysis
Histopathological analysis was performed on paraffin-embedded slices that were 5 μm thick. The sections were stained with hematoxylin and eosin for one to two minutes at room temperature after being fixed in 10% neutral buffered formalin for twenty-four hours. After that, the slices were examined using a Leica Microsystems GmbH light microscope.
Data analysis
The data collected were analyzed using an Excel spreadsheet (Microsoft Excel 2016). Descriptive statistics were applied to summarize the results and results were presented as mean ± standard deviation, range, frequencies, and percentages.
Results
Clinical findings
This study included 5 EMC cases, of which 4 (80%) were females and a male (20%). The average age of the patients was 56 ± 9.38 years. All the patients were non-smokers. Two patients (40%) had no significant past medical history, while a patient (20%) had hypertension, another patient (20%) had diabetes, and another (20%) had both hypertension and diabetes (Table 1). Two patients (40%) presented with right post-auricular swelling, one patient (20%) presented with right submandibular swelling, and 2 patients (40%) were incidental findings. On ultrasonography, tumor sizes ranged from 1.1 cm to 4.1 cm, with a mean size of 2.54 ± 1.25 cm. One patient (20%) underwent left submandibular gland excision, 1 (20%) underwent right submandibular gland excision, 2 (40%) underwent right superficial parotidectomy, and 1 (20%) underwent total conservative parotidectomy with supraomohyoid lymph node dissection. During follow up none of the patients developed recurrent swelling at the site of the previous operation. The follow-up ranged from 1 to 70 months, with a mean duration of 24 ± 28.92 months, with no cases of recurrence (Table 2).
|
Case no. |
Age |
Sex |
Medical History |
Surgical History |
Family History |
Smoker |
Duration |
|
1 |
68 |
Female |
HTN, DM |
cholecystectomy |
Negative |
Not smoker |
1 year |
|
2 |
52 |
Female |
Negative |
D&C |
Negative |
Not smoker |
- |
|
3 |
48 |
Female |
Negative |
Negative |
Negative |
Not smoker |
1 year |
|
4 |
48 |
Female |
HTN |
Appendectomy |
Negative |
Not smoker |
- |
|
5 |
64 |
Male |
DM |
Negative |
Negative |
Not smoker |
1 year |
| HTN, Hypertension; DM, Diabetes Mellitus; D&C, dilatation and curettage | |||||||
|
No. cases |
Presentation |
Examination |
Tumor size on ultrasound |
Ultrasound findings |
Milan system |
Operation |
Histological diagnosis |
Outcome |
|
1 |
Right post-auricular swelling |
Hard mass |
35*19*16mm |
Salivary gland nodule located in the right parotid gland |
Not Performed |
Right superficial parotidectomy |
Epithelial-myoepithelial carcinoma |
No recurrence, Alive |
|
2 |
Incidental findings |
Small mobile mass |
11*9*6mm |
Mixed solid nodule in superficial part of right parotid gland |
Milan IV-A |
Right superficial parotidectomy |
Epithelial-myoepithelial carcinoma |
No recurrence, Alive |
|
3 |
Right submandibular swelling |
Mobile fixed mass |
23*19*13mm |
Salivary gland nodule located in the right submandibular gland |
Not Performed |
Right submandibular gland excision |
Epithelial-myoepithelial carcinoma |
No recurrence, Alive |
|
4 |
Incidental findings |
Mobile fixed mass |
41*30*28mm
|
Salivary gland nodule occupying left submandibular gland |
Milan IV-A |
Left submandibular gland excision |
Epithelial-myoepithelial carcinoma |
No recurrence, Alive |
|
5 |
Right post-auricular swelling |
Irregular, firm mobile mass |
17*14*13mm |
Mixed solid nodule in superficial part of right parotid gland |
Milan VI |
Total conservative parotidectomy + supraomohyoid Lymph node dissection |
Epithelial-myoepithelial carcinoma |
No recurrence, Alive |
Pathological findings
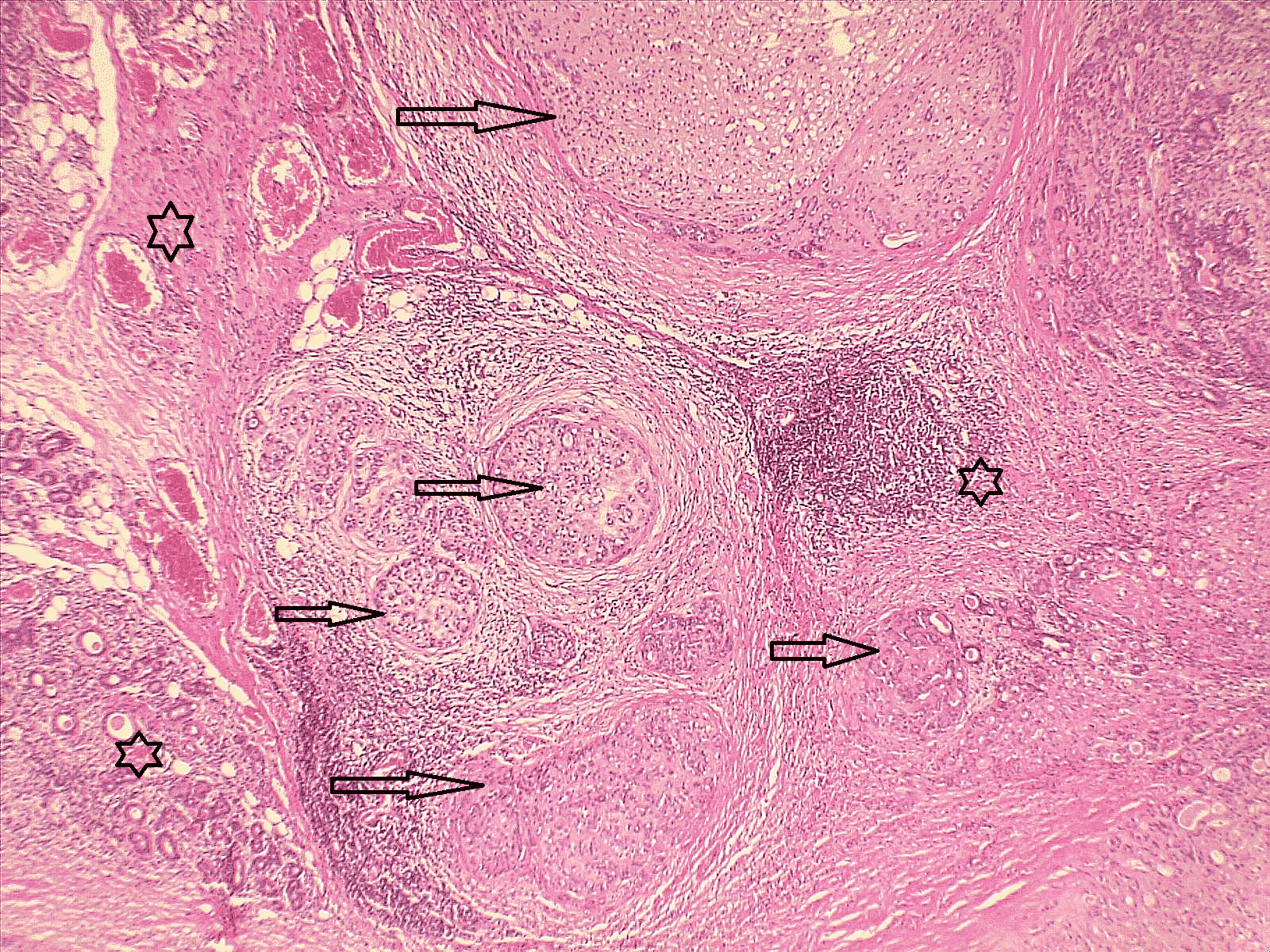
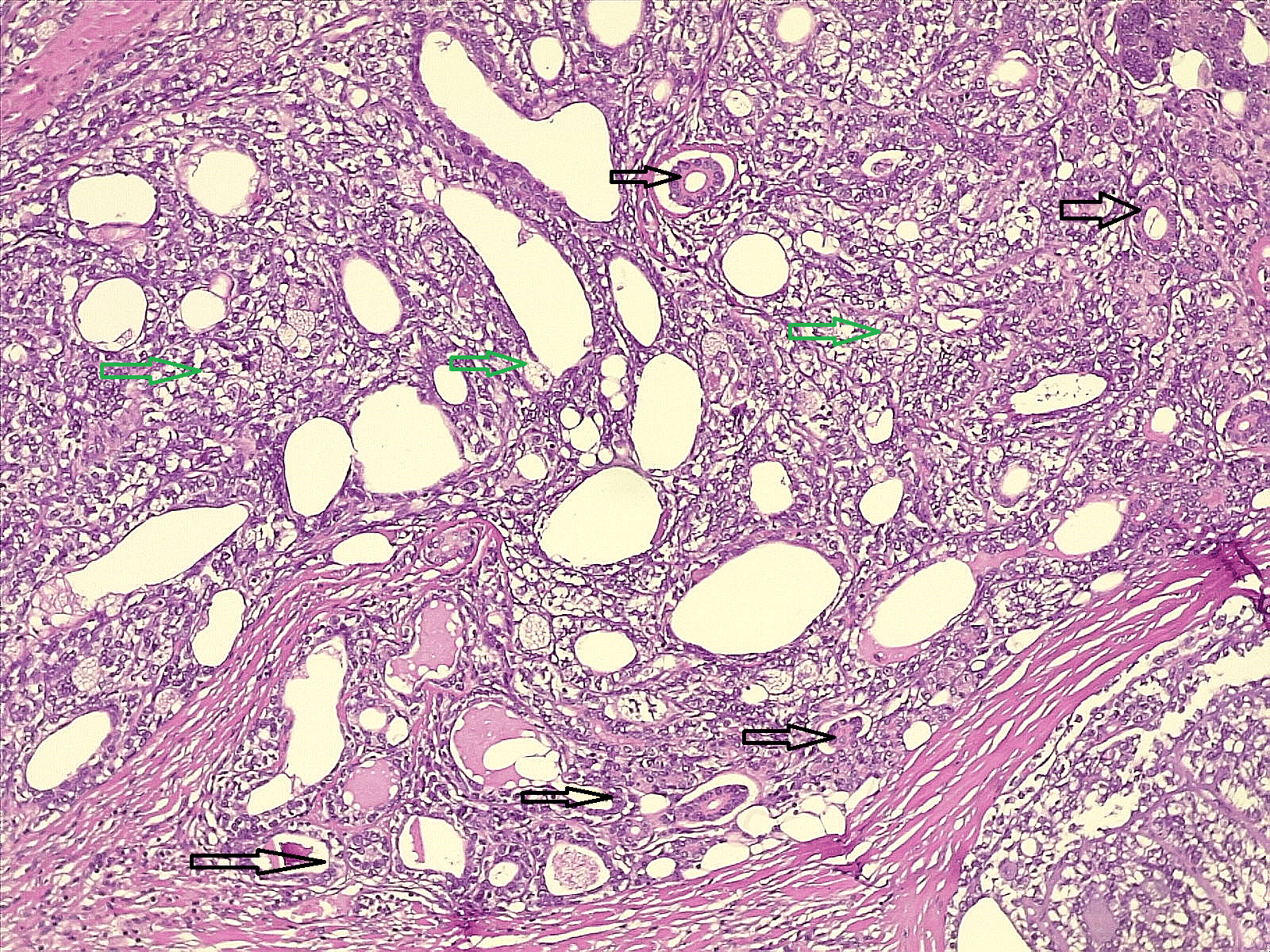
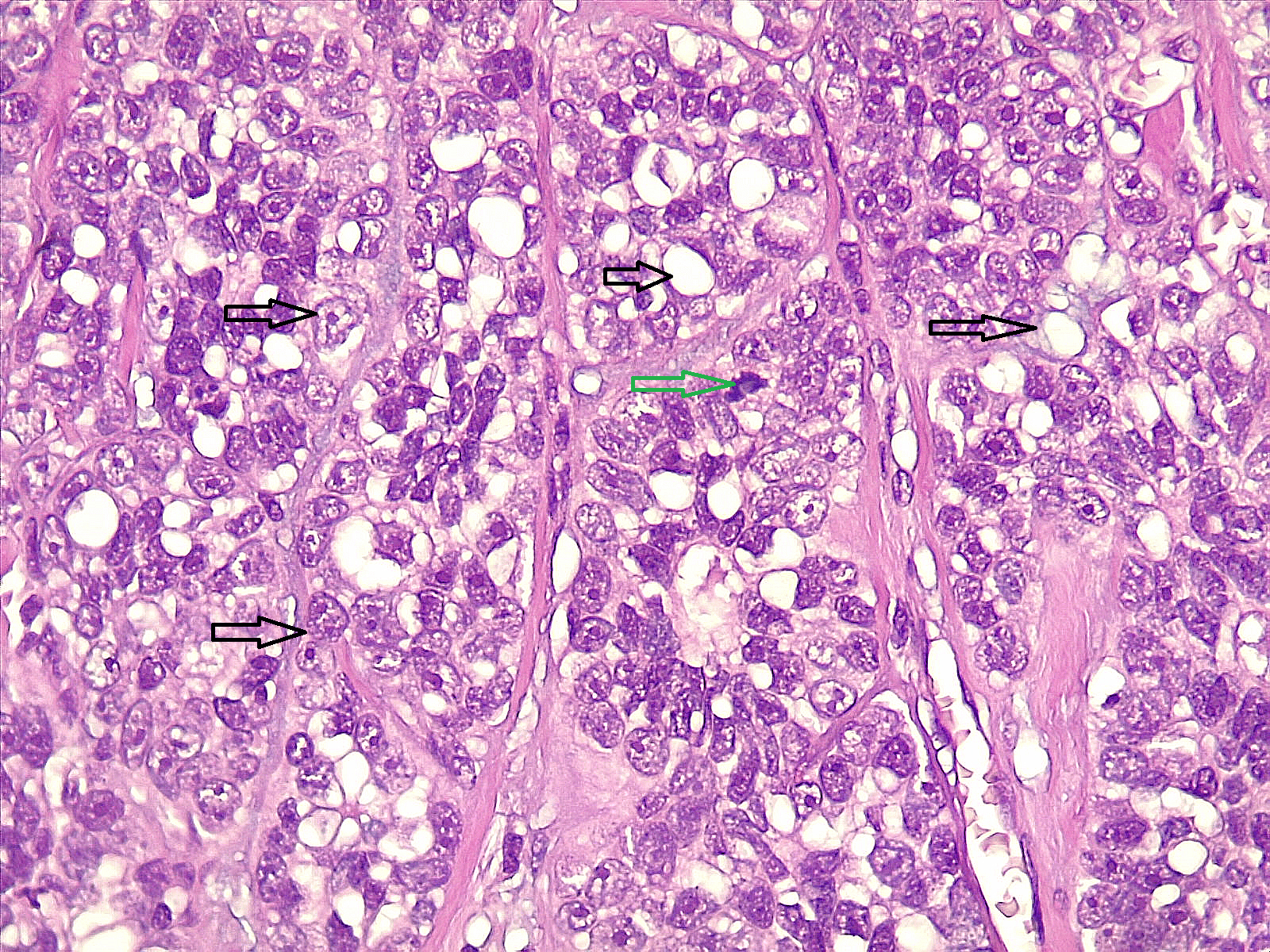
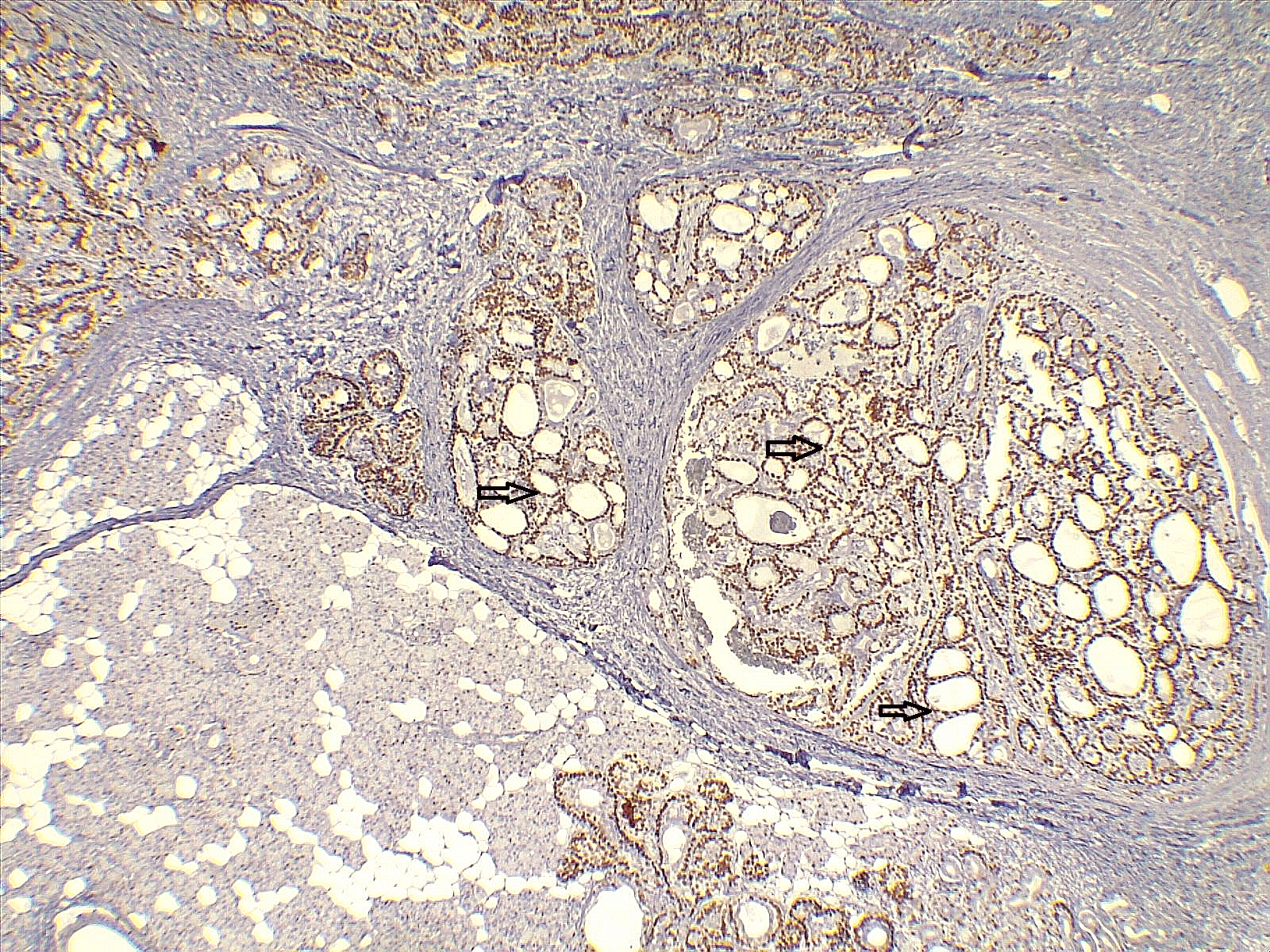
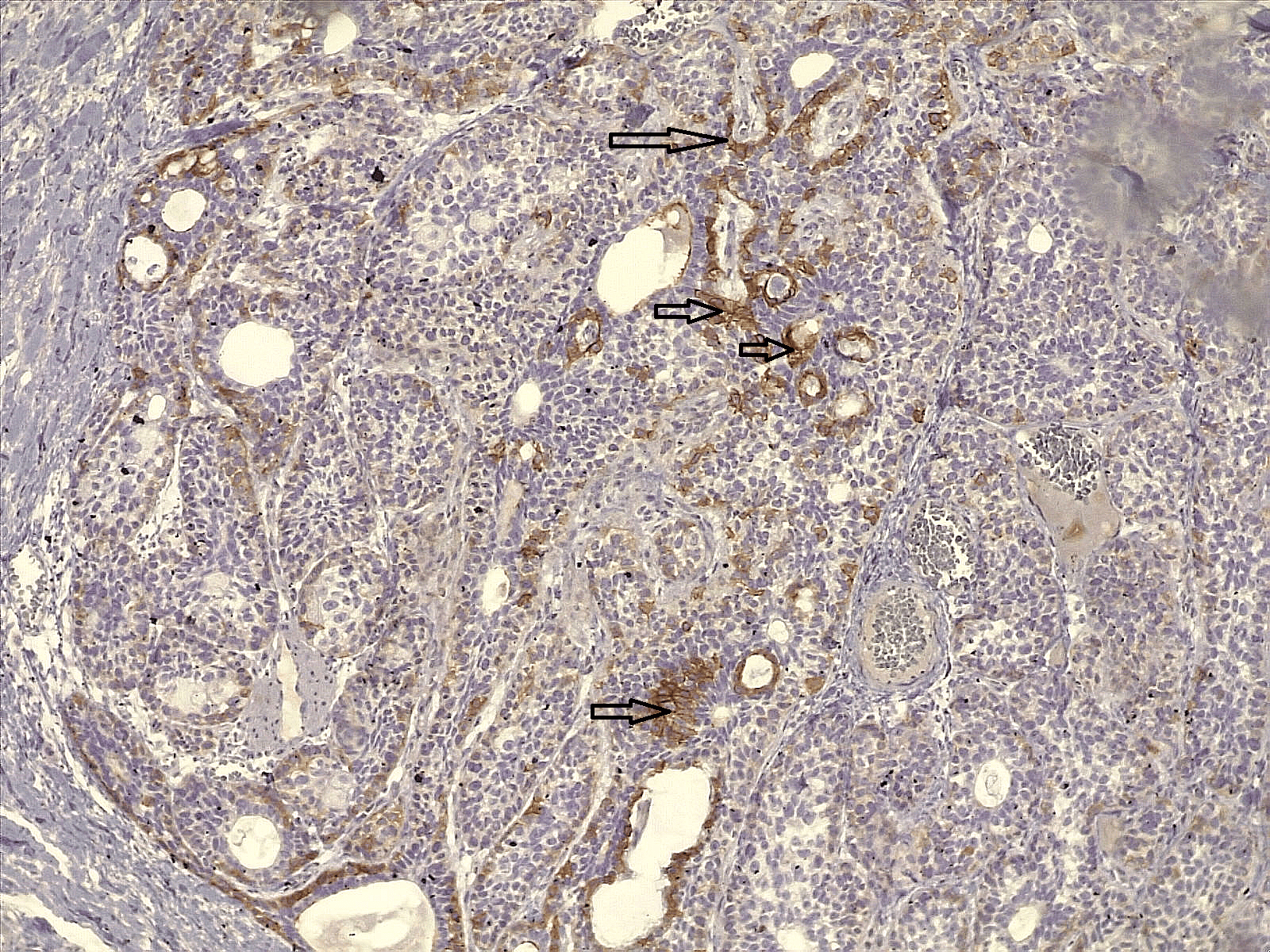
Histopathological examination revealed epithelial-myoepithelial carcinoma in all 5 patients. The average maximum tumor length on histopathological examination was 2.22 ± 0.91 cm. Four tumors (80%) exhibited an infiltrative growth pattern, while 1 (20%) had a pushing pattern. All 5 patients (100%) showed negative lymph node involvement. Three tumors (60%) had free margins, while 2 tumors (40%) had invasive margins. In terms of tumor necrosis visibility, 2 tumors (40%) had no visible necrosis, 2 tumors (40%) had visible focal necrosis, and 1 tumor (20%) had visible intra-tumoral and central necrosis (Table 3). Microscopically, a low-power view demonstrated nodules of a lobulated mass infiltrating into the adjacent salivary gland parenchyma (Figure 1). At higher magnification, the tumors were composed of two distinct populations of cells, some arranged as small ducts lined by epithelial cells, with another population composed of atypical cells with abundant clear cytoplasm (Figure 2). Further high-power examination highlighted these atypical clear cells with the presence of a mitotic figure within the field (Figure 3). Immunohistochemical analysis showed P63 immune stain highlighting the myoepithelial cells (Figure 4), while DOG1 immune stain demonstrated an apical membranous staining pattern in some of the epithelial cells (Figure 5).
|
Case No. |
Tumor size |
Tumor capsule |
Tumor border (growth pattern) |
Necrosis |
Lymph-vascular invasion |
Perineural invasion |
Margins |
Lymph nodes involvement |
Pathological stage (AJCC) |
|
1 |
2.5 cm |
Not present |
Infiltrative |
Not seen |
Not seen |
Seen |
Invasive |
Not involved |
pT2 N0 |
|
2 |
0.9 cm |
Not Available |
Infiltrative |
Not seen |
Not seen |
Seen |
Free |
Not involved |
pT1 N0 |
|
3 |
3 cm |
Not Available |
Infiltrative |
Seen, focal |
Not seen |
Not seen |
Free |
Not involved |
pT2 N0 R0 |
|
4 |
3 cm |
Not Available |
Infiltrative |
Seen, focal |
Not seen |
Seen |
Invasive |
Not involved |
pT2 N0 |
|
5 |
1.7 cm |
Present, intact |
Pushing |
Seen, intra-tumoral, central |
Not seen |
Not seen |
Free |
Not involved |
pT1 N0 |
| AJCC, American Joint Committee on Cancer | |||||||||
Discussion
The clinical behavior of EMC reflects its low-grade malignant nature, though significant morbidity can result from local recurrence [6]. Data from the Armed Forces Institute of Pathology indicates that EMC constitutes approximately 1% of all salivary epithelial neoplasms and nearly 2% of malignant salivary epithelial neoplasms [1].
Epithelial-myoepithelial carcinoma predominantly affects older adults, with a peak incidence in the sixth and seventh decades of life, and demonstrates a female predominance [6]. In the present series, 80% of patients were female, with a mean age of 56 ± 9.38 years. These findings are consistent with the published literature. A previous analysis of 246 cases reported 57.32% females and 42.68% males, with a mean age of 63.8 ± 15.4 years [8]. Another review of 16 cases found a female-to-male ratio of approximately 1.6:1, with a mean age of 61.5 years [6].
Additional reports describing patients aged 64 and 65 years further support the predilection for older adults [3,4]. The slight differences in age and sex distribution between the present study and larger series may be attributable to the small sample size of the current cohort.
Regarding clinical presentation, EMC most commonly manifests as a painless mass [4]. In the current study, 60% of patients presented with painless swelling, while 40% were detected incidentally. Corio et al. reported that among nine patients with recorded symptoms, four (44.4%) presented with an asymptomatic swelling [6]. Taş et al. noted that their patient presented with a two-month history of a painless mass that had recently increased in size [3]. These observations reinforce the typically indolent clinical course of EMC, which may contribute to delayed detection in some cases.
Histologically, EMC demonstrates a multinodular growth pattern with variable proportions of ductal and myoepithelial cells [1]. In the present series, histologic grading was available for four cases (80%), of which 60% were classified as low-grade and 20% as intermediate-grade. Vázquez et al. reported that 32.93% of cases in their study were of low histologic grade (grades I and II), although histologic grade was unavailable for 60.57% of cases [8]. High-grade transformation, though rare (occurring in approximately 3.4% to 6.5% of cases), is associated with aggressive clinical behavior and poorer prognosis [9].
Surgical management remains the cornerstone of treatment for EMC [2]. In this series, treatment strategies were individualized based on tumor location and extent, with patients undergoing either parotidectomy or submandibular gland excision. Vázquez et al. reported that nearly all patients (97.1%) in their study underwent surgery, while 41.1% received adjuvant radiotherapy; however, no survival benefit was noted for patients who received radiotherapy compared with those who did not [8]. Adequate surgical resection with negative soft-tissue margins is considered the minimum recommended therapy because of the high risk of local recurrence [1,4].
Margin status remains a clinically significant parameter in EMC, given its recognized potential for local recurrence [1,6]. In the current series, invasive margins were identified in 40% of cases. Previous studies have reported high rates of local recurrence, including cases with multiple recurrences over prolonged follow-up periods and eventual distant metastasis [2,6]. The reported local recurrence rate approaches 50% in some series [4]. Despite the presence of invasive margins in 40% of the cases in this series, no recurrences were observed during the follow-up period, which ranged from 1 to 70 months (mean 24 ± 28.92 months).
Lymph node involvement and distant metastases are considered uncommon in EMC [1]. In the present series, no nodal or distant metastases were identified. A previous study reported distant metastases at diagnosis in only 4.5% of cases [8]. Friedrich and Donath, however, documented a case with multiple distant metastases to the lung and foot, demonstrating that although rare, metastatic spread remains a recognized clinical possibility [2]. Another report similarly reported one patient who developed metastasis to the kidney and subsequently died [6]. In a cytologic study of myoepithelial cell-rich neoplasms, observed that pleomorphism, coarse chromatin, prominent nucleoli, mitotic figures, and necrosis were seen exclusively in malignant specimens, including one case of EMC, providing useful cytologic criteria for distinguishing benign from malignant myoepithelial lesions [10].
The present study has several limitations. First, the follow-up duration was relatively short for assessing long-term recurrence and survival. Second, molecular and genetic analyses were not performed. Third, the small sample size limits the generalizability of the current series’ findings.
Conclusion
Epithelial-myoepithelial carcinoma requires histopathological evaluation for accurate diagnosis, and complete surgical excision offers favorable short-term outcomes. Further studies are needed to better define its clinical characteristics and outcomes.
Declarations
Conflicts of interest: The authors have declared that no competing interests exist.
Ethical approval: In accordance with our institution's oral policy, retrospective case series involving anonymized histopathological material and de-identified patient data do not require formal ethical approval.
Patient consent (participation and publication): Informed consent for publication was obtained from the patients.
Funding: The present study received no financial support.
Acknowledgements: None to be declared.
Authors' contributions: AMS, HOA, ROM, MLF, and IJH were significant contributors to the conception of the study, the literature search for related studies, managed the cases, and performed critical revision. AMA was a pathologist who contributed to the pathological analysis. STS and HAM contributed to the conception of the idea, data collection and interpretation, and critical revision. RSA, SHQ, SHH, DHH. AAQ contributed to the conception of the idea, literature review, table preparation, and critical revision. LLH contributed to the conception of the idea, literature review, and drafting of the manuscript. All authors have read and approved the final version of the manuscript.
Use of AI: ChatGPT-4.5 was used to assist with language refinement and improve the overall clarity of the manuscript. All content was thoroughly reviewed and approved by the authors, who bear full responsibility for the final version.
Data availability statement: The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
- Politi M, Robiony M, Avellini C, Orsaria M. Epithelial-myoepithelial carcinoma of the parotid gland: Clinicopathological aspect, diagnosis and surgical consideration. Annals of maxillofacial surgery. 2014;4(1):99-102. doi:10.4103/2231-0746.133085
- Friedrich RE, Donath K. Epithelial-myoepithelial carcinoma of the parotid gland with multiple distant metastases: a case report. Journal of Oral and Maxillofacial Surgery. 2000;58(6):690-4. doi:10.1016/S0278-2391(00)90171-X
- Taş A, Yağız R, Koten M, Karasalihoğlu AR, Altaner Ş. A case of epithelial-myoepithelial carcinoma of the parotid gland. The Turkish Journal of Ear Nose and Throat. 2003;10(4):171-4. doi:N/A
- Silvers AR, Som PM, Brandwein M. Epithelial-myoepithelial carcinoma of the parotid gland. American journal of neuroradiology. 1996;17(3):560-2.
- Palmer RM. Epithelial-myoepithelial carcinoma: an immunocytochemical study. Oral surgery, oral medicine, oral pathology. 1985;59(5):511-5. doi:10.1016/0030-4220(85)90093-3
- Corio RL, Sciubba JJ, Brannon RB, Batsakis JG. Epithelial-myoepithelial carcinoma of intercalated duct origin: a clinicopathologic and ultrastructural assessment of sixteen cases. Oral Surgery, Oral Medicine, Oral Pathology. 1982;53(3):280-7. doi:10.1016/0030-4220(82)90304-8
- Fahmi H. Kakamad, Shvan H. Mohammed, Berun A. Abdalla, Dahat A. Hussein, Zuhair D. Hammood, Suhaib H. Kakamad, et al. Non-Recommended Publishing Lists: Strategies for Detecting Deceitful Journals. Barw Medical Journal. 2026;4(1):13-21. doi:10.58742/bmj.v4i1.227
- Vázquez A, Patel TD, D’Aguillo CM, Abdou RY, Farver W, Baredes S, Eloy JA, Park RC. Epithelial-myoepithelial carcinoma of the salivary glands: an analysis of 246 cases. Otolaryngology--Head and Neck Surgery. 2015;153(4):569-74. doi:10.1177/0194599815594788
- Nakaguro, M., & Nagao, T. Epithelial–Myoepithelial Carcinoma. Surgical Pathology Clinics, 2021;14(1), 97–109. doi:10.1016/j.path.2020.10.002
- Darvishian F, Lin O. Myoepithelial cell‐rich neoplasms: Cytologic features of benign and malignant lesions. Cancer Cytopathology: Interdisciplinary International Journal of the American Cancer Society. 2004;102(6):355-61. doi:10.1002/cncr.20642

This work is licensed under a Creative Commons Attribution 4.0 International License.