
Torsades de Pointes Following Ondansetron Administration: A Case Report with literature review

Abstract
Introduction
Ondansetron blocks human ether-à-go-go-related gene (hERG) potassium channels, causing QT prolongation and risk of torsades de pointes (TdP). Despite its widespread use, TdP following a standard intravenous dose is rarely reported. This report presents a case of a 40-year-old female who developed TdP after receiving an 8 mg intravenous dose of ondansetron.
Case Presentation
A 40-year-old female with no significant past medical history presented with vomiting and diarrhea. Approximately 30 minutes after receiving 8 mg of intravenous ondansetron, she developed TdP requiring cardioversion. Laboratory results revealed mild hypokalemia (3.12 mmol/L). Post-event troponin elevation and Grade I diastolic dysfunction suggested transient myocardial involvement. She was stabilized with potassium replacement and supportive care, with full recovery.
Literature Review
Five cases of ondansetron-induced TdP were reviewed. Patient ages ranged from 41 to 60 years, one case (20%) involved oral administration and four cases (80%) involved intravenous administration. Doses ranged from standard 4 mg to cumulative 36 mg infusions, with QTc intervals reaching up to 653 ms. Presenting events included TdP, ventricular tachycardia, and cardiac arrest. Symptom resolution and recovery were achieved in all cases following medical intervention and electrolyte correction.
Conclusion
This case highlights that standard-dose ondansetron can precipitate TdP in physiologically unstable patients.
Introduction
Prolongation of the QT interval on electrocardiography (ECG) is a well-recognized precursor to torsades de pointes (TdP), a potentially fatal arrhythmia that may degenerate into ventricular fibrillation and sudden cardiac death [1]. Drug-induced QT prolongation remains one of the most common causes of post-marketing drug withdrawal or restriction and continues to represent a major safety concern in clinical practice [2]. Hospitalized patients are thought to be at particularly high risk due to the frequent presence of multiple predisposing factors, including electrolyte abnormalities, structural heart disease, bradycardia, and concomitant use of other QT-prolonging medications [1,2].
Ondansetron, a selective 5-HT3 receptor antagonist and first-line antiemetic, has been shown to prolong the QT interval and has been associated with ventricular arrhythmias [3,4]. In 2011, the United States Food and Drug Administration (FDA) issued a safety warning regarding QT prolongation and the potential risk of TdP associated with ondansetron, particularly at higher intravenous doses [4,5]. Ondansetron inhibits the rapid component of the delayed rectifier potassium current (IKr) mediated by the human ether-à-go-go-related gene (hERG) potassium channel, resulting in delayed ventricular repolarization and QT interval prolongation [2]. Beyond the risk of ventricular tachycardia, the pharmacological impact of ondansetron on the heart is multifaceted and can manifest through various other electrophysiological disturbances. While its primary association is with the prolongation of the QT interval, the drug has also been linked to supraventricular arrhythmias and acute changes in myocardial function [6]. Despite regulatory warnings regarding QT prolongation, TdP following standard-dose ondansetron remains rarely reported, especially in cases associated with reversible electrolyte disturbances [4].
This report presents a case of a 40-year-old female who developed TdP after receiving an 8 mg intravenous dose of ondansetron. This report was prepared following the CaReL guidelines, and all references were carefully evaluated to ensure they met the eligibility criteria [7,8].
Case Presentation
A 40-year-old woman presented to the emergency department with diarrhea, repeated vomiting, and reduced oral intake. She had no significant medical history and was on no medications. Family history was noncontributory. She denied smoking, illicit substance use, or prior cardiac disease.
On presentation, she was alert, oriented, and in no acute distress. Her vital signs were within normal limits: temperature, 36.8 °C; blood pressure, 110/65 mmHg; heart rate, 90 beats/min; respiratory rate, 17 breaths/min; and oxygen saturation, 98% on room air. Cardiovascular examination revealed a regular rate and rhythm with no murmurs or rubs. Initial lung auscultation was normal. Abdominal examination was unremarkable, and there was no peripheral edema.
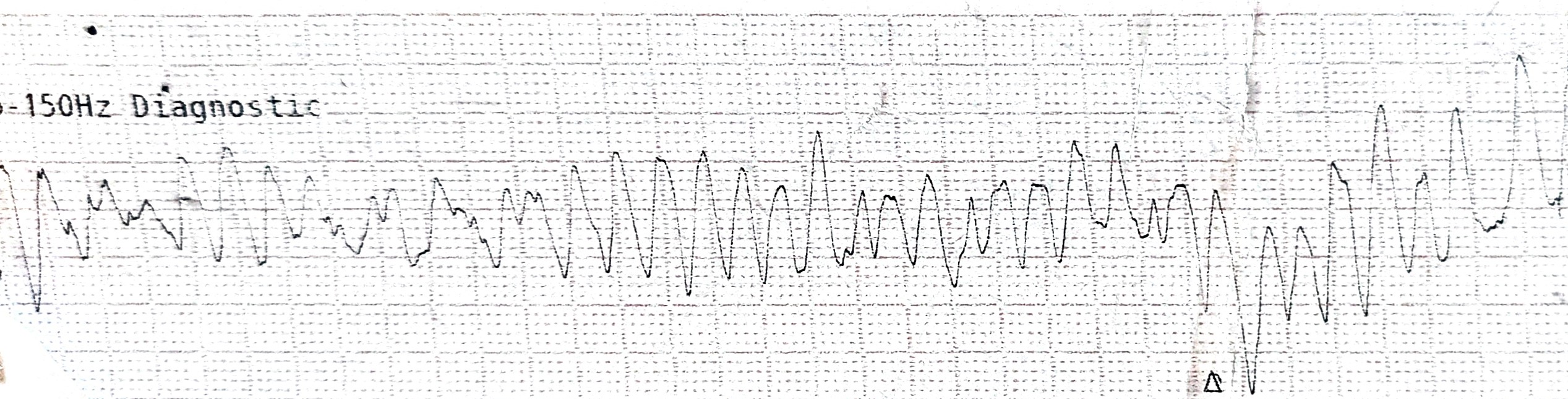
Blood samples for electrolytes were obtained on arrival at 22:00. While awaiting the results, the patient received 8 mg intravenous ondansetron at 22:10 for nausea and vomiting. Approximately 30 minutes later (22:40), she developed a cardiac arrhythmia. ECG demonstrated polymorphic ventricular tachycardia consistent with TdP (Figure 1). Immediate DC cardioversion was performed, with restoration of sinus rhythm.
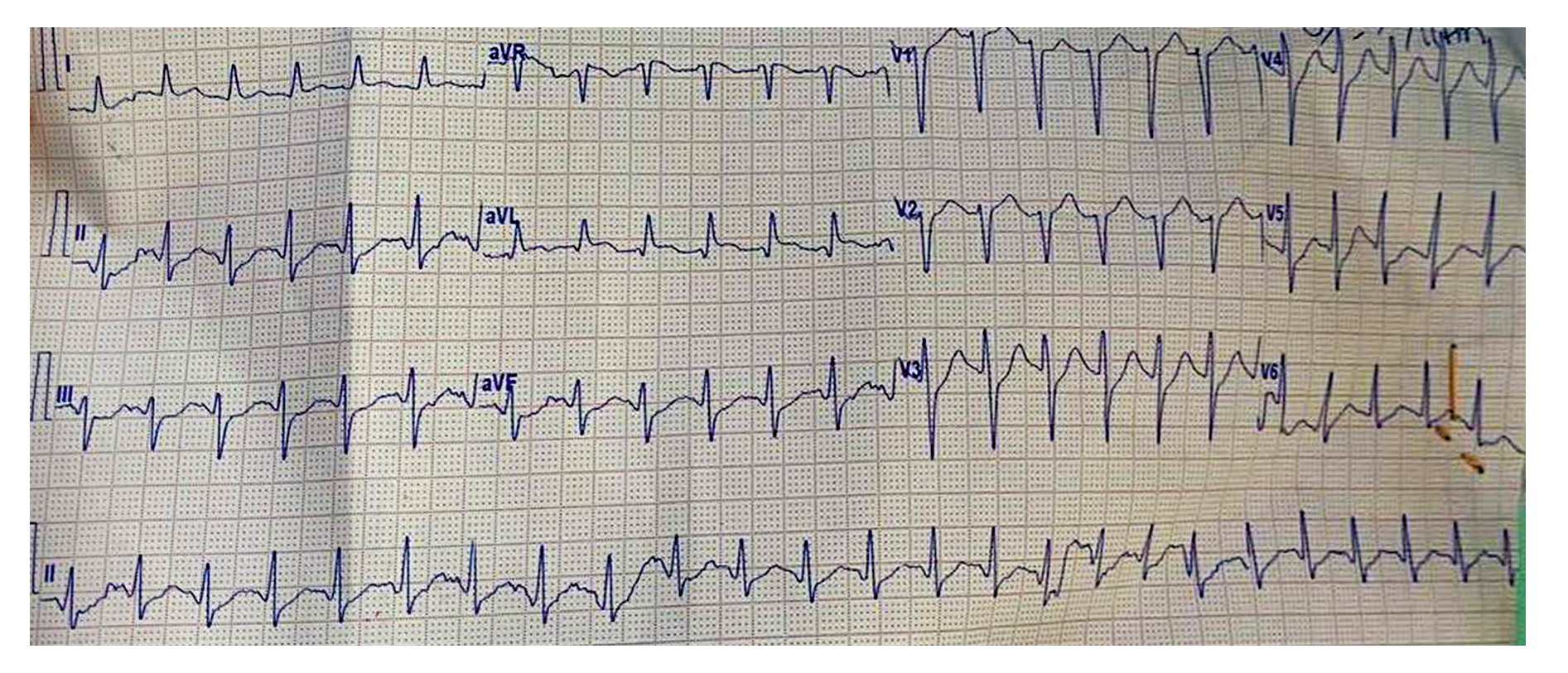
Ten minutes after the event, ECG showed a QTc of 489 ms and supraventricular tachycardia (Figure 2). Initial laboratory results (drawn pre-ondansetron, reported at 23:18) showed sodium 138.9 mmol/L (reference, 135–150), potassium 3.12 mmol/L (reference, 3.5–5.0), ionized calcium 1.14 mmol/L (reference, 1.10–1.35), chloride 108.3 mmol/L (reference, 94–110), and pH 7.435 (reference, 7.35–7.45), confirming hypokalemia.
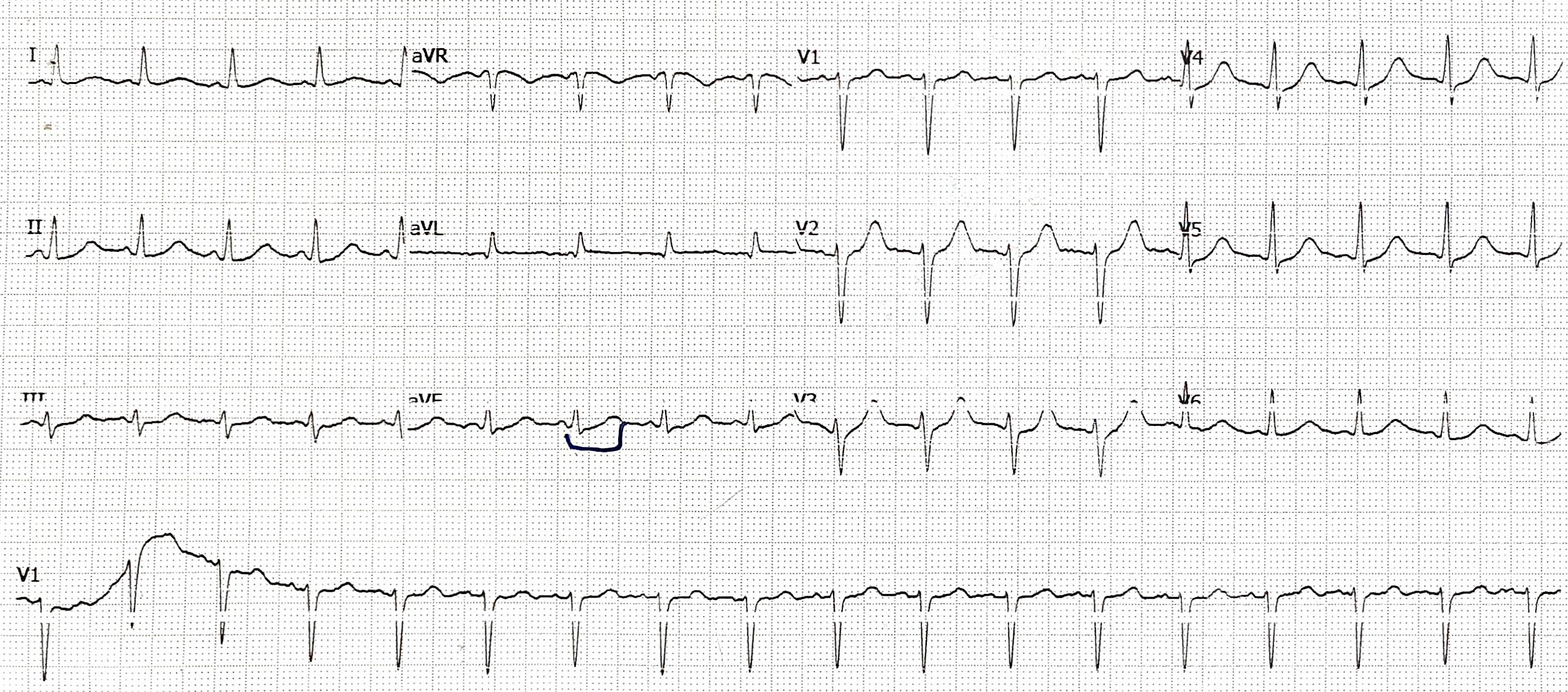
During the post-cardioversion period, the patient developed tachypnea, tachycardia, hypotension, and bilateral fine crepitations on auscultation. High-sensitivity troponin T at 01:10 was 109.8 ng/L, increasing to 208.8 ng/L at 03:00. Repeat electrolytes and renal function tests at 03:05 showed potassium 3.06 mmol/L with normal renal function, indicating persistent hypokalemia. Intravenous potassium replacement (20 mEq in 500 mL over 3 hours) was initiated. Follow-up electrolytes at 09:59 demonstrated potassium 3.7 mmol/L, and repeat ECG showed sinus tachycardia (Figure 3).
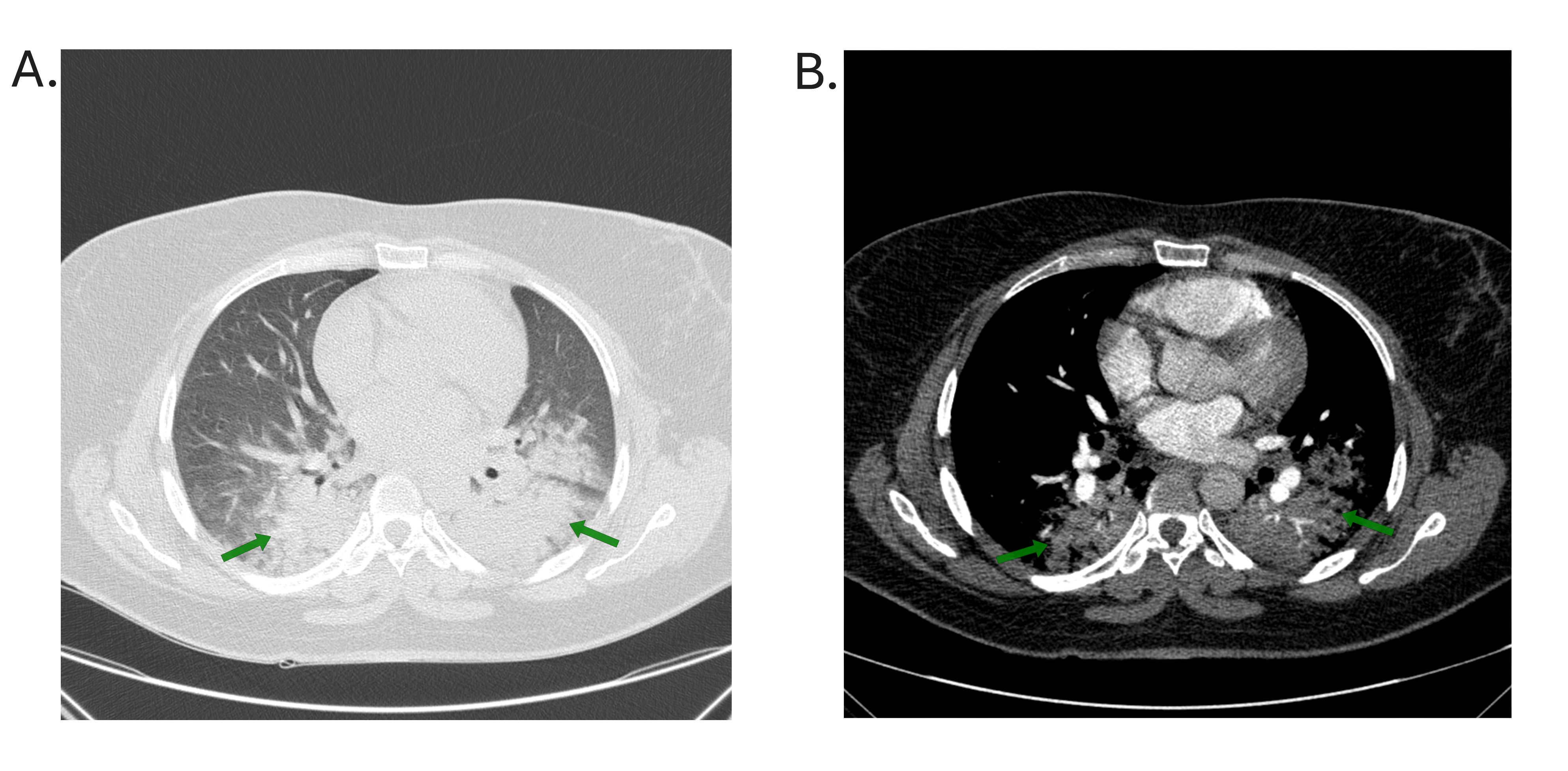
Approximately 11 hours after the TdP event, CT coronary angiography showed normal coronary anatomy. Fifteen hours after the event, CT chest with intravenous contrast revealed bilateral consolidation suggestive of pulmonary edema and aspiration pneumonia (Figure 4). On day 1, serum magnesium was normal; calcium was low at 7.8 mg/dL (reference, 8.9–10.0). On day 3, transthoracic echocardiography revealed normal cardiac structure and systolic function, with Grade I diastolic dysfunction. The patient's condition gradually stabilized with supportive care and electrolyte correction, and she was discharged in stable condition.
Discussion
Ondansetron-induced TdP, although uncommon, is a recognized adverse effect of the drug. The underlying mechanism involves blockade of the rapid component of the delayed rectifier potassium current via inhibition of hERG potassium channels, which delays ventricular repolarization and prolongs the QT interval [2,3]. This electrophysiological disturbance creates a substrate for early afterdepolarizations, which can trigger polymorphic ventricular tachycardia [9]. In the present case, TdP occurred after a single standard 8 mg intravenous dose, suggesting a role for additional contributing factors.
Five cases of ondansetron-induced TdP were reviewed. A search of PubMed/MEDLINE and Google Scholar up to 2026, identified these cases. The mean age of the patients was 49.2 years (range: 41–60 years). Female sex was predominant, accounting for four cases (80%), while one case (20%) was male. Regarding the route of administration, intravenous ondansetron was used in four cases (80%), and oral administration in one case (20%). Doses ranged from a standard 4 mg single dose to a cumulative infusion of 36 mg. Marked QTc prolongation was observed in all cases, with recorded intervals ranging from 543 ms to 653 ms. Arrhythmic events included TdP (100% of cases), ventricular tachycardia (three cases, 60%), and cardiac arrest (three cases, 60%). Despite the severity of these events, all five patients (100%) recovered fully following interventions such as advanced cardiovascular life support (ACLS), magnesium sulfate administration, and electrolyte correction (Table 1) [3,4,10,11].
|
Author (y) [Ref] |
N |
Mean age (year) |
Gender |
Indication |
Dose |
Route |
QTc after ondansetron |
Arrhythmic event |
Management |
Outcome |
|
|
Tafish et al. (2025) [10] |
1 |
43 |
F |
Nausea & vomiting |
8mg |
IV |
582ms |
Polymorphic VF, TdP & cardiac arrest |
ACLS |
Recovered |
|
|
Orozco et al. (2023) [4] |
1 |
41 |
F |
Nausea & vomiting |
4 mg |
IV |
653ms |
TdP & Cardiac arrest |
ACLS |
Recovered |
|
|
Patel et al. (2019) [11] |
1 |
60 |
F |
Nausea |
4 mg |
Oral |
NA |
VT & TdP |
Magnesium sulfate 2g IV, and oral magnesium oxide 400mg |
Recovered |
|
|
Lee et al. (2017) [3] |
2 |
51 |
F & M |
Nausea & vomiting (both) |
36mg & 12mg |
IV (both) |
610ms & 543ms |
VT, TdP, cardiac arrest & VT |
ACLS & Electrolyte correction |
Resuscitated and recovered & recovered |
|
|
Ref, reference; F, female; M, male; IV, intravenous; VT, ventricular tachycardia; TdP, Torsades de pointes; ACLS, advanced cardiovascular life support |
|||||||||||
In this case, the patient developed TdP in the setting of hypokalemia (3.06 mmol/L), likely caused by ongoing potassium loss from vomiting and diarrhea. Female sex and electrolyte abnormalities, particularly hypokalemia and hypomagnesemia, are well-recognized predisposing factors for drug-induced QT prolongation [1]. Torsades de pointes in the reported case developed after an 8 mg intravenous dose, whereas Hafermann et al. reported that a 4 mg intravenous dose did not significantly prolong the QT interval, even in high-risk cardiovascular patients [2]. In contrast, Patel et al. described TdP following a single 4 mg orally disintegrating tablet in the presence of risk factors [11]. Ondansetron may also unmask latent congenital Long QT Syndrome (LQTS) when combined with electrolyte abnormalities [12]. Together, these findings suggest that the arrhythmogenic risk of ondansetron depends less on the dose alone and more on the presence of coexisting risk factors.
Large-scale retrospective data contrast with these individual reports. Nuttall et al. found no instances of TdP among over 32,000 surgical patients receiving 4 mg perioperative ondansetron [5], and a similarly low incidence of ventricular arrhythmias (0.003%) has been reported in the pediatric population [13]. However, these reassuring figures derive largely from elective or stable populations and may not apply to acute medical settings, such as the emergency department presentation in the current case, where patients are physiologically unstable and often have ongoing electrolyte losses. Consistent with this, cardiac arrests have been reported in two children following ondansetron administration [9].
Furthermore, the cardiovascular effects of ondansetron may extend beyond TdP. Atrial fibrillation has been reported following ondansetron administration, suggesting that its effects on cardiac serotonin receptors may disrupt rhythm stability more broadly [6]. More severe presentations, including cardiac arrest and transient cardiomyopathy, have also been described [10]. This is consistent with the present case, in which post-event troponin elevation and Grade I diastolic dysfunction on echocardiography raised the possibility of transient myocardial involvement following the arrhythmic event.
Additionally, symptomatic sinus bradycardia has also been reported following intravenous ondansetron, attributed to its influence on both parasympathetic and sympathetic limbs of the autonomic nervous system [14]. This bradycardic effect may further predispose vulnerable patients to TdP, as bradycardia is itself a known risk factor for QT-related arrhythmias [11].
In our report, the main limitations were the absence of a baseline ECG prior to ondansetron administration, which precluded establishing the baseline QTc or excluding undiagnosed congenital long QT syndrome, and the lack of a magnesium level at the time of the event, given that hypomagnesemia is an independent risk factor for TdP.
Conclusion
This case highlights that standard-dose ondansetron can precipitate life-threatening TdP in physiologically unstable patients, particularly when potentiated by electrolyte abnormalities like hypokalemia.
Declarations
Conflicts of interest: The authors have no conflicts of interest to disclose.
Ethical approval: Not applicable.
Patient consent (participation and publication): Written informed consent was obtained from the patient for publication.
Funding: This research did not receive any specific funding from public, commercial, or not-for-profit funding agencies. The work was performed as part of the routine clinical and academic activities of the authors' institutions.
Acknowledgements: None to be declared.
Authors' contributions: SHA, SFA, DHBM, FJA, ANQ, and KFH managed the case and performed critical revision. SHT was a radiologist who contributed to the radiological assessment. ONM and PKA contributed to the literature review, table preparation, and critical revision. LLH contributed to the conception of the idea, the literature review, and the drafting of the manuscript. All authors have read and approved the final version of the manuscript.
Use of AI: Claude Opus-4.7 was used to assist with language refinement and improve the overall clarity of the manuscript. All content was thoroughly reviewed and approved by the authors, who bear full responsibility for the final version.
Data availability statement: The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
- Trinkley KE, Lee Page R, Lien H, Yamanouye K, Tisdale JE. QT interval prolongation and the risk of torsades de pointes: essentials for clinicians. Current medical research and opinion. 2013 ;29(12):1719-26. doi:10.1185/03007995.2013.840568
- Hafermann MJ, Namdar R, Seibold GE, Page 2nd RL. Effect of intravenous ondansetron on QT interval prolongation in patients with cardiovascular disease and additional risk factors for torsades: a prospective, observational study. Drug, healthcare and patient safety. 2011 :53-8. doi:10.2147/dhps.s25623
- Lee DY, Trinh T, Roy SK. Torsades de pointes after ondansetron infusion in 2 patients. Texas Heart Institute Journal. 2017 ;44(5):366-9. doi:10.14503/THIJ-16-6040
- Orozco BS, Lee SC, Fuchs RT, Fushianes GD, Cole JB. QT prolongation, torsades des pointes, and cardiac arrest after 4 mg of IV ondansetron. The American Journal of Emergency Medicine. 2023 ;68:214-e3. doi:10.1016/j.ajem.2023.04.003
- Nuttall GA, Voogd SC, Danke H, Warner PA, Oyen LJ, Marienau MS, et al. The incidence of torsades de pointes with peri‐operative low‐dose ondansetron administration. Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy. 2022 ;42(4):292-7. doi:10.1002/phar.2668
- Kasinath NS, Malak O, Tetzlaff J. Atrial fibrillation after ondansetron for the prevention and treatment of postoperative nausea and vomiting: a case report. Canadian journal of anaesthesia. 2003 ;50(3):229-31. doi:10.1007/BF03017789
- Prasad S, Nassar M, Azzam AY, García-Muro-San José F, Jamee M, Sliman RK, et al. CaReL Guidelines: A Consensus-Based Guideline on Case Reports and Literature Review (CaReL). Barw Med J. 2024;2(2):13–19. doi:10.58742/bmj.v2i2.89
- Abdullah HO, Abdalla BA, Kakamad FH, Ahmed JO, Baba HO, Hassan MN, et al. Predatory Publishing Lists: A Review on the Ongoing Battle Against Fraudulent Actions. Barw Med J. 2024;2(2):26–30. doi:10.58742/bmj.v2i2.91
- Brenner SM, Boucher J. Fatal cardiac arrest in 2 children: possible role of ondansetron. Pediatric Emergency Care. 2016 ;32(11):779-84. doi:10.1097/PEC.0000000000000317
- Tafish R, Elsayed R, Alsolamy S, Aljuaid W, Yaseen R, Kuhail A. Ondansetron-induced cardiac arrest and cardiomyopathy with successful reversal: a case report. AME Case Report. 2025 ;9:122. doi:10.21037/acr-25-3
- Patel E, Rosemond D, Afzal A. Ondansetron induced torsades de pointes. Clinical Case Reports. 2019 ;7(8):1557. doi:10.1002/ccr3.2251
- Sethi P, Treece J, Pai V, Onweni C. Long QT Syndrome Unveiled by a Fatal Combination of Medications and Electrolyte Abnormalities. Cureus. 2017 ;9(8). doi:10.7759/cureus.1581
- Moeller JR, Gummin DD, Nelson TJ, Drendel AL, Shah BK, Berger S. Risk of ventricular arrhythmias and association with ondansetron. The Journal of Pediatrics. 2016 ;179:118-23. doi:10.1016/j.jpeds.2016.08.058
- Moazzam MS, Nasreen F, Bano S, Amir SH. Symptomatic sinus bradycardia: A rare adverse effect of intravenous ondansetron. Saudi Journal of Anaesthesia. 2011 ;5(1):96-7. doi:10.4103/1658-354X.76492

This work is licensed under a Creative Commons Attribution 4.0 International License.