
Clinicopathological Characteristics and Survival Outcomes of Breast Cancer in Young Women

Abstract
Introduction
Breast cancer in young women, defined as diagnosis before 40 years of age. It is characterized by poorer outcomes compared with older patients. Regional data on the disease in the Middle Eastern population remain limited. This study focused on the clinicopathological profile of young women with breast cancer.
Methods
This retrospective, single-center cohort study was conducted between February 2018 and February 2025. Demographic, clinical, pathological, treatment, and follow-up data were extracted from electronic medical records. Inclusion criteria were women under 40 years diagnosed with primary breast cancer. Patients with incomplete records or without surgical treatment were excluded.
Results
A total of 564 patients with a median age of 36 years (IQR: 5) were included. A breast mass was the predominant chief complaint (85.5%), and 74.7% presented within 3 months. Median tumor size was 25 mm. Invasive ductal carcinoma was the predominant subtype (88%). Triple-negative breast cancer was identified in 73 patients (12.9%), of which 76.1% were Grade III (p<0.001). Negative estrogen and progesterone receptor status was significantly associated with Grade III (p<0.001). Wide local excision was performed in 67.0% of cases. Overall survival was 98.5% at 60 months.
Conclusion
High tumor grade was significantly associated with triple negative breast cancer, ER-negative, and PR-negative status, but not with HER2 status. Symptom duration showed no association with tumor size. Ki-67 was significantly higher in Grade III tumors, reinforcing the aggressive phenotype of breast cancer in young women.
Introduction
Breast cancer in young women (BCYW) is defined as a diagnosis before 40 years of age and constitutes approximately 7% of all breast cancer cases. Among women aged 25 to 39 years, breast cancer is one of the frequently diagnosed malignancies. The incidence of BCYW has been rising steadily, with metastatic disease at diagnosis also increasing [1,2].
The pathogenesis of BCYW is multifactorial, driven by an interplay of heritable, hormonal, and biological influences. A significant proportion of cases is attributable to germline mutations in high-penetrance genes, including BRCA1, BRCA2, PALB2, TP53, PTEN, STK11, and CDH1 [3], while the tumor microenvironment exhibits distinct features such as increased collagen deposition and altered immune infiltration [4]. Hormonal and reproductive factors, including early menarche, nulliparity, and oral contraceptive use, alongside lifestyle factors such as alcohol consumption, smoking, and obesity, further contribute to disease risk [5]. Together, these factors underline the aggressive biology and poor prognosis that characterize this population [4].
Dedicated regional studies in the Middle Eastern populations focusing exclusively on breast cancer in women under 40 remain sparse, with existing Iranian and Saudi cohorts limited by modest sample sizes [6,7]. Iraqi data on this population remains limited, with existing reports representing early foundational work that warrants validation through larger dedicated studies [8]. Breast cancer is now the leading cause of cancer death among women under 40 years [9]. Young women are more likely to be diagnosed with aggressive subtypes, including triple-negative breast cancer (TNBC) and human epidermal growth factor receptor 2 (HER2)-enriched disease, and more advanced stage, contributing to poorer survival outcomes compared to older women [1,10]. These distinct clinical and psychosocial challenges, including fertility and family planning concerns, make this population a critical focus for dedicated research [3].
This study aims to report the clinicopathological features of breast cancer among young women based on a single-center experience. Only peer-reviewed data were included after careful verification of all references [11].
Methods
Study design
This retrospective, single-center, cohort study was conducted over seven years, from February 2018 to February 2025. All patients provided informed consent, including permission to use anonymized clinical data for research and publication purposes.
Data source
Clinical data were extracted from electronic medical records. Collected variables included demographic characteristics, patients' medical and surgical histories, family history (FHX), presenting symptoms, preoperative imaging findings, diagnostic findings, management, outcomes, and follow-up.
Eligibility criteria
The study included female patients diagnosed with primary breast cancer who were younger than 40 years at the time of diagnosis. Patients with incomplete medical records or those who did not undergo surgical intervention were excluded from the analysis.
Procedure
Patients underwent surgery under general anesthesia in the supine position following standard skin preparation and antiseptic protocols. Surgical access was achieved using either elliptical or Stewart incisions, depending on tumor location and breast anatomy. Procedures included wide local excision, simple mastectomy, nipple/skin-sparing mastectomy, or modified radical mastectomy, based on tumor extent and clinical staging. Axillary management consisted of either lymph node sampling or complete axillary dissection when indicated. In all cases, the long thoracic and thoracodorsal nerves were carefully preserved. Meticulous hemostasis was ensured, and a closed-suction drain (Redivac) was placed routinely. Wound closure was performed in anatomical layers according to standard surgical practice.
Statistical analysis
Data were initially recorded in Microsoft Excel (2024) and subsequently analyzed using the Statistical Package for Social Sciences (SPSS), version 25. Categorical variables were analyzed using Fisher's exact test, with Cramer's V calculated as a measure of effect size for significant associations. Continuous variables were summarized as medians with interquartile ranges (IQRs) because the data were non-normally distributed according to the Shapiro-Wilk test. Continuous variables were compared between two independent groups using the Mann–Whitney U test, and their relationships were evaluated using Spearman’s correlation coefficient. Overall survival was estimated using the Kaplan-Meier method. Results were presented as frequencies and percentages for categorical variables. A p-value of <0.05 was considered statistically significant.
Results
A total of 564 patients with a median age of 36 years (IQR: 5) were included. The most common chief complaint was a breast mass (482 patients, 85.5%), followed by breast pain (61, 10.8%), axillary mass (12, 2.1%), and nipple discharge (9, 1.6%). Symptom duration was within 1 month in 164 patients (29.1%), 1 to 3 months in 257 (45.6%), 3 to 6 months in 99 (17.5%), and > 6 months in 44 (7.8%). Overall, 421 patients (74.7%) sought medical consultation within three months of symptom onset. Among 563 patients, 419 (74.4%) reported no FHX of malignancy, while 144 (25.6%) had at least one affected family member. Within the latter group, the two most reported malignancies were breast cancer in 81 patients (56.3%) and gastrointestinal tract malignancies in 32 (22.2%). Nulliparity was observed in 168 patients (29.8%), while 396 (70.2%) were parous. A history of lactation was reported in 323 patients (57.3%), while 241 (42.7%) had never lactated (Table 1).
|
Variables |
Frequency / Percentage |
|
Patient Demographics |
|
|
Age, median (IQR), years |
36 (5) |
|
Marital Status |
|
|
Married Single Widowed |
493 (87.4%) 64 (11.4%) 7 (1.2%) |
|
Past Medical History |
|
|
No significant comorbidities Hypertension Hypothyroidism Other conditions |
530 (94.0%) 14 (2.5%) 6 (1.1%) 14 (2.4%) |
|
Family History of Cancer (n=563) |
|
|
Negative Positive Breast cancer Gastrointestinal tract malignancy Prostate cancer Other |
419 (74.4%) 144 (25.6%) 81 (56.3%) 32 (22.2%) 6 (4.2%) 25 (17.3%) |
|
Parity |
|
|
Nulliparous Parous 1 child 2 children 3 children 4 children ≥5 children |
168 (29.8%) 396 (70.2%) 26 (4.6%) 118 (20.9%) 125 (22.2%) 84 (14.9%) 43 (7.6%) |
|
Lactation |
|
|
Yes No |
323 (57.3%) 241 (42.7%) |
|
Duration of Lactation |
|
|
< 1 year 1–3 years 4–6 years ≥7 years |
28 (8.7%) 139 (43.0%) 115 (35.6%) 41 (12.7%) |
|
Clinical Presentation |
|
|
Breast mass Breast pain Axillary mass Nipple discharge |
482 (85.5%) 61 (10.8%) 12 (2.1%) 9 (1.6%) |
|
Symptom Duration Before Presentation |
|
|
< 1 month 1–3 months >3–6 months > 6 months |
164 (29.1%) 257 (45.6%) 99 (17.5%) 44 (7.8%) |
| IQR: Interquartile Range | |
Regarding tumor size assessed by ultrasound, data were available for 537 patients, with a median size of 25 mm (IQR: 19.5; range: 4–110 mm). Tumors ≤20 mm accounted for 192 cases (35.8%), those measuring 21–50 mm for 283 cases (52.7%), and those >50 mm for 62 cases (11.5%). Breast Imaging-Reporting and Data System (BIRADS) classification results were available for 557 patients: 388 patients (69.7%) were classified as BIRADS 5 (U5), 141 patients (25.3%) as BIRADS 4 (U4), 27 patients (4.8%) as BIRADS 3 (U3), and 1 patient (0.2%) as BIRADS 2 (U2) (Table 2).
|
Variables |
Frequency / Percentage |
|
Tumor Laterality |
|
|
Left Right |
282 (50.0%) 282 (50.0%) |
|
Tumor Site on Ultrasound (n=550) |
|
|
Upper Outer Quadrant Upper Inner Quadrant Lower Outer Quadrant Upper central Lateral central Lower central Medial central Multiple quadrants / Central |
196 (35.6%) 112 (20.4%) 68 (12.4%) 53 (9.6%) 33 (6.0%) 21 (3.8%) 15 (2.7%) 52 (9.5%) |
|
Tumor Size on Ultrasound (n=537) |
|
|
Median (IQR), mm Range, mm ≤20 mm 21–50 mm > 50 mm |
25 (19.5) 4–110 192 (35.8%) 283 (52.7%) 62 (11.5%) |
|
Ultrasound BIRADS Classification (n=557) |
|
|
BIRADS 2 BIRADS 3 BIRADS 4 BIRADS 5 |
1 (0.2%) 27 (4.8%) 141 (25.3%) 388 (69.7%) |
| IQR: Interquartile Range | |
Core biopsy data (n=555) demonstrated invasive ductal carcinoma (IDC) as the predominant subtype (86.4%), followed by ductal carcinoma in situ (4.3%), invasive lobular carcinoma (3.2%), and invasive mammary carcinoma (1.8%). Fine-needle aspiration results of the lymph nodes were available for 515 patients, with positive findings in 255 (49.5%), negative in 246 (47.8%), and inconclusive in 14 (2.7%). In total, 73 patients (12.9%) had TNBC. Estrogen receptor (ER) status (n=318) was positive in 67.6% and negative in 32.4%, while progesterone receptor (PR) status (n=310) was positive in 58.4% and negative in 41.6%. HER2 status (n=309) was negative in 76.7%, positive in 22.7%, and equivocal in 0.6%. Ki-67 (n=231) had a median of 37% (IQR: 39), with high expression (>30%) in 57.6%, low (<20%) in 24.2%, and intermediate (20–30%) in 18.2%. Tumor grade (n=459) was mainly Grade II (51.9%) and Grade III (40.9%), with Grade I in 7.2%.
Surgical management included wide local excision in 67.0%, simple mastectomy in 23.0%, modified radical mastectomy in 6.0%, and nipple/skin-sparing mastectomy in 3.9%. Sentinel lymph node biopsy was performed in 46.8%, and axillary lymph node dissection in 49.6%. Postoperative histopathology revealed IDC in 88%, ductal carcinoma in situ in 4.4%, invasive lobular carcinoma in 2.3%, invasive mammary carcinoma in 2.1%, and other subtypes in 3.2%. Adjuvant therapy included radiotherapy in 86.9%, chemotherapy in 85.1%, and hormone therapy in 76.6% (Table 3).
|
Variables |
Frequency / Percentage |
|
Fine Needle Aspiration (n=515) |
|
|
Positive Negative Inconclusive |
255 (49.5%) 246 (47.8%) 14 (2.7%) |
|
Core Biopsy (n=555) |
|
|
Invasive Ductal Carcinoma Ductal Carcinoma In Situ Invasive Lobular Carcinoma Invasive Mammary Carcinoma Other malignant subtypes |
479 (86.4%) 24 (4.3%) 18 (3.2%) 10 (1.8%) 24 (4.3%) |
|
Receptor Status |
|
|
Estrogen receptor (n=318) |
|
|
Positive Negative |
215 (67.6%) 103 (32.4%) |
|
Progesterone Receptor (n=310) |
|
|
Positive Negative |
181 (58.4%) 129 (41.6%) |
|
Human Epidermal Growth Factor Receptor 2 (n=309) |
|
|
Positive Negative Equivocal |
70 (22.7%) 237 (76.7%) 2 (0.6%) |
|
Triple Negative Disease |
73 (12.9%) |
|
Ki-67 (n=231) |
|
|
Median (IQR), % Range, % Low (<20%) Intermediate (20–30%) High (>30%) |
37 (39) 2–90 56 (24.2%) 42 (18.2%) 133 (57.6%) |
|
Tumor Grade (n=459) |
|
|
Grade I Grade II Grade III |
33 (7.2%) 238 (51.9%) 188 (40.9%) |
|
Surgical Procedures |
|
|
Wide Local Excision Simple Mastectomy Modified Radical Mastectomy Nipple and Skin Sparing Mastectomy |
378 (67.0%) 130 (23.0%) 34 (6.0%) 22 (3.9%) |
|
Axillary Surgery (n=562) |
|
|
Sentinel Lymph Node Biopsy Axillary Lymph Node Dissection Level I & II Axillary Lymph Node Dissection Level I, II & III Axillary Lymph Node Dissection Level I No axillary sampling |
263 (46.8%) 244 (43.4%) 32 (5.7%) 3 (0.5%) 20 (3.6%) |
|
Postoperative Histopathology |
|
|
Invasive Ductal Carcinoma Ductal Carcinoma In Situ Invasive Lobular Carcinoma Invasive Mammary Carcinoma Other subtypes |
496 (88%) 25 (4.4%) 13 (2.3%) 12 (2.1%) 18 (3.2%) |
|
Adjuvant Therapy* |
|
|
Radiation therapy Chemotherapy Hormone therapy |
490 (86.9%) 480 (85.1%) 432 (76.6%) |
|
IQR: Interquartile Range *Each patient could receive more than one therapy. |
|
The median follow-up duration was 30 months (IQR: 42 months). Over the follow-up period, 533 patients (94.5%) were alive without distant metastasis, 9 (1.6%) developed metastatic disease, and 5 (0.9%) developed contralateral breast cancer. In total, 17 patients (3.0%) succumbed to the disease. (Table 4).
|
Variables |
Frequency / Percentage |
|
Follow-up Duration |
|
|
Median (IQR), months < 12 months 12–24 months 24–48 months 48–72 months ≥72 months |
30 (42) 67 (11.9%) 131 (23.2%) 155 (27.5%) 142 (25.2%) 69 (12.2%) |
|
Recurrence and Metastasis |
|
|
Alive, no evidence of distant metastasis Metastatic disease Bone Brain Brain and liver Lung Unspecified site Contralateral breast cancer Mortality |
533 (94.5%) 9 (1.6%) 1 (0.2%) 1 (0.2%) 1 (0.2%) 1 (0.2%) 5 (0.9%) 5 (0.9%) 17 (3.0%) |
| IQR: Interquartile Range | |
Triple-negative breast cancer, ER, and PR status were all significantly associated with tumor grade (p<0.001). Among 67 TNBC patients with available grade data, 51 (76.1%) were Grade III and 16 (23.9%) were Grade I–II, whereas among 221 non-TNBC patients, 150 (67.9%) were Grade I–II and 71 (32.1%) were Grade III (Cramer’s V=0.376). Among 92 ER-negative patients, 62 (67.4%) showed Grade III, and 30 (32.6%) showed Grade I–II, while among 197 ER-positive patients, tumors in 136 (69.0%) were Grade I–II, and 61 (31.0%) were Grade III (Cramer’s V=0.343). Among 120 PR negative patients, 75 (62.5%) were Grade III and 45 (37.5%) were Grade I–II, while in 166 PR positive patients, tumors in 118 (71.1%) cases were Grade I–II and 48 (28.9%) were Grade III (Cramer’s V=0.335). No significant association was found between HER2 status and tumor grade (p=0.777) (Table 5).
|
Variables |
Tumor grade |
Triple Negative Status |
Estrogen Receptor |
Progesterone Receptor |
HER2 Status |
||||
|
Yes** |
No |
Positive |
Negative |
Positive |
Negative |
Positive |
Negative |
||
|
Tumor Grade |
Grade I-II |
16 (23.9%) |
150 (67.9%) |
136 (69.0%) |
30 (32.6%) |
118 (71.1%) |
45 (37.5%) |
37 (56.1%) |
127 (58.3%) |
|
Grade III |
51 (76.1%) |
71 (32.1%) |
61 (31.0%) |
62 (67.4%) |
48 (28.9%) |
75 (62.5%) |
29 (43.9%) |
91 (41.7%) |
|
|
P-value# |
<0.001 |
<0.001 |
<0.001 |
0.777 |
|||||
|
Cramer's V |
0.376 |
0.343 |
0.335 |
|
|||||
|
Family History of Breast Cancer |
Positive |
— |
— |
44 (54.3%) |
18 (22.2%) |
34 (54.8%) |
28 (45.2%) |
10 (16.9%) |
49 (83.1%) |
|
Negative |
— |
— |
171 (68.4%) |
85 (34.0%) |
147 (59.3%) |
101 (40.7%) |
60 (22.8%) |
154 (58.6%) |
|
|
P-value# |
— |
0.643 |
0.661 |
0.290 |
|||||
|
# Fisher's Exact Test HER2: Human Epidermal Growth Factor Receptor 2 —: Not applicable for this comparison ** A total of 73 cases were triple-negative, while tumor grade data were available for 67 cases. |
|||||||||
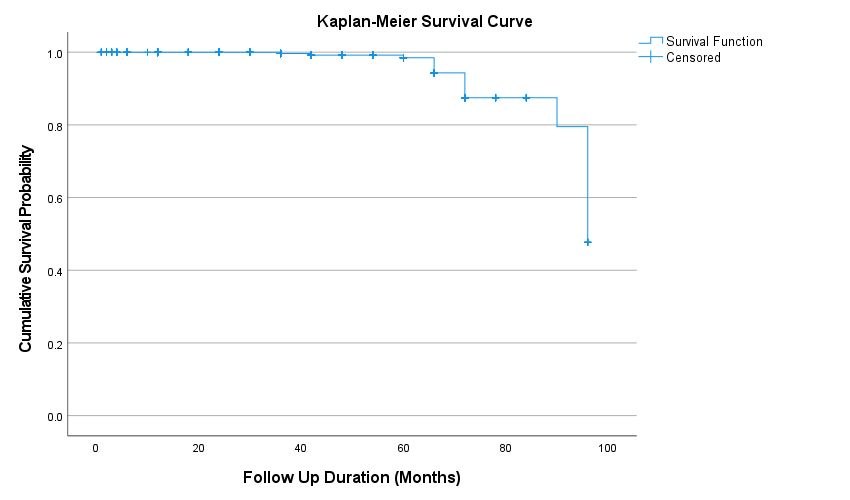
No significant associations were observed between FHX of breast cancer and receptor status (ER p=0.643, PR p=0.661, HER2 p=0.290), or between symptom duration and tumor size at presentation (Spearman’s r=-0.029, p=0.509). Ki-67 was significantly higher in Grade III tumors than in Grade I–II tumors (Mann-Whitney U=3632.500, Z=-4.576, p<0.001), with mean ranks of 131.08 and 92.06, respectively (Table 6). Kaplan-Meier survival analysis showed 5-year and 6-year survival rates of 98.5% and 87.5%, respectively (Figure 1).
|
Variables |
Tumor Grade |
N |
Mean Rank |
Test Statistic |
p-value* |
|
Ki-67 |
Grade I-II |
125 |
92.06 |
U=3632.5, Z=-4.576 |
<0.001 |
|
Grade III |
91 |
131.08 |
|||
|
Age at presentation |
Grade I-II |
272 |
233.31 |
U=24531.5, Z=-0.648 |
0.517 |
| * Mann-Whitney U Test | |||||
Discussion
Breast cancer in young women is more often diagnosed symptomatically rather than through screening, as routine mammographic screening programs typically do not include this age group [7]. A palpable breast mass is the predominant presenting complaint, followed less commonly by nipple discharge, breast pain, axillary mass, and skin changes [12]. The diagnostic work-up is complicated by dense breast tissue, which limits mammographic sensitivity and necessitates greater reliance on ultrasound, with magnetic resonance imaging serving as an important adjunct [7]. Imaging features frequently demonstrate masses with irregular shapes, spiculated margins, and microlobulated or angular features, often classified as BIRADS 4 or 5 [7]. Given the higher prevalence of germline pathogenic variants in this age group [3], genetic testing has become an increasingly integral component of the diagnostic work-up, with approximately one-third of tested patients identified as carriers in a recent young breast cancer cohort [7].
In the present study, the median age at diagnosis was 36 years (IQR: 5), aligning with regional young breast cancer cohorts, including Moghani et al. in Iran (65.6% aged 31–35 years) and Alhaidary et al. in Saudi Arabia (83.4% aged 30–40 years), as well as El Saghir et al. in Lebanon (median 36 years) [6,7,13]. Regarding the symptom profile, a breast mass was the predominant presentation in the current cohort (85.5%), consistent with findings reported by Eugênio et al. in a cohort of 120 women aged <40 years, where a palpable nodule was identified as the principal clinical finding (52.5% as an isolated finding and 20.8% in association with other signs such as papillary retraction, skin thickening, and edema) [14].
Presentation within three months of symptom onset was documented in 74.7% of patients, with 25.3% presenting beyond three months. The median tumor size on ultrasound (25 mm) was smaller than the median of 55 mm reported by Anwar et al. and the mean of 36.3 mm documented by Alhaidary et al. [7,15], but was comparable to the range of mean tumor sizes (21–35 mm) reported by Sopik et al. across seven international young breast cancer cohorts [16]. Despite variation in symptom duration, no significant correlation was identified between symptom duration and tumor size at presentation (p=0.509). This finding suggests that tumor size in young breast cancer patients may not be primarily determined by patient-related delay. This interpretation aligns with the work of Unger-Saldaña et al., who found that while patients aged ≤40 years had an increased risk of diagnostic delay (odds ratio 1.69, p=0.029), this association disappeared after adjusting for lack of cancer suspicion by the first physician consulted. Notably, misdiagnosis occurred in 53.6% of young patients compared to only 31.5% of older patients (p<0.001) [17]. Costa et al. further emphasized that the advanced disease frequently observed at presentation in young breast cancer patients reflects the faster intrinsic tumor growth rate characteristic of this age group, which compounds the impact of any diagnostic delay [18].
In this study, a FHX of breast cancer was documented in 14.4%, a prevalence approximately two-fold higher than the 7.6% reported for FHX of breast or ovarian cancer in a study by Anwar et al. about young breast cancer patients [15]. The 5.7% prevalence of gastrointestinal malignancy among family members is noteworthy, as familial clustering of breast and gastrointestinal cancers has been linked to syndromic causes of early-onset breast cancer, including Li-Fraumeni (TP53), Peutz-Jeghers (STK11), and hereditary diffuse gastric cancer (CDH1) syndromes [3]. These findings support current recommendations that genetic counseling and testing should be offered to young breast cancer patients, as a negative FHX does not exclude an underlying heritable predisposition [3].
Triple-negative breast cancer was strongly associated with high grade, with 76.1% classified as Grade III (p<0.001). This is consistent with Tzikas et al., in which 91.4% of patients under 40 years with primary TNBC were shown to have Grade III tumors compared with 80.2% of those over 74 years (p=0.006) [19]. A similar pattern was reported by Murphy et al., where adolescent and young adult patients aged 15–39 years had a higher prevalence of TNBC disease than adults aged 40–49 years (21.2% vs 13.8%, p<0.001), with the most aggressive features concentrated in those aged 15–29 years [10]. Estrogen receptor-negative and PR-negative tumors were significantly associated with Grade III in the present cohort (67.4% and 62.5%, respectively; p<0.001). Zhu et al., in their systematic review, observed a higher proportion of ER-negative, high-grade tumors in young women, supporting the present findings [20]. However, no comparable data on PR status alone, in relation to tumor grade, were identified in the reviewed literature. In contrast, no significant association was found between HER2 status and tumor grade in the present study (p=0.777). This differs from Ayatollahi et al., who found that HER2 amplification was significantly correlated with younger patient age, higher tumor grade, lymph node metastasis, larger tumor size, and poorer survival outcomes [21].
A high Ki-67 index (>30%) was identified in 57.6% of patients in the present study, with a median value of 37%, and Ki-67 values were significantly higher in Grade III tumors than in Grade I–II tumors (p<0.001). This is consistent with Abubakr et al., which showed a strong positive correlation between Ki-67 and tumor grade (Spearman's r=0.68, p<0.001), with mean Ki-67 rising from 15.8% in Grade 1 to 23.2% in Grade 2 and 34.7% in Grade 3 [22]. A similar proliferative index has been reported by Lee et al. (mean Ki-67 41.9%, with higher values in those who developed recurrence: 57.6% vs 37.0%, p=0.056) [23]. These findings reinforce the link between young age at diagnosis and intrinsically aggressive tumor biology [20].
Wide local excision was the most frequently performed procedure in the present cohort (67.0%), followed by mastectomy in 33.0%. This breast-conserving rate is notably higher than that reported in regional and international young breast cancer cohorts, including Anwar et al. (radical or modified radical mastectomy was 84%) and Abulkhair et al. (mastectomy was 44.9%; lumpectomy was 25.8%) [15,24]. However, it is more consistent with the rate of breast-conserving surgery (BCS) reported by El Saghir et al. (51%) and Lee et al. (74.5%) [13,23]. The higher proportion of BCS in the present cohort likely reflects the smaller tumor size at presentation observed in this study. Invasive ductal carcinoma was identified as the predominant histological subtype (88%), in line with the finding of El Saghir et al., where IDC accounted for 94.3% of cases among patients aged ≤40 years [13]. Invasive lobular carcinoma was uncommon (2.3%), closely mirroring the 1.3% reported in the previous study and reinforcing the well-documented underrepresentation of this subtype in young breast cancer populations. Ductal carcinoma in situ was recorded in 4.4% of patients, identical to the proportion reported by El Saghir et al. [13].
Short-term survival was favorable, with Kaplan–Meier estimates of overall survival at 98.5% at 5 years and 87.5% at 6 years. While direct comparisons are limited by the relatively short median follow-up of 30 months, these findings are broadly consistent with prior reports, including El Saghir et al. (89.4%) and Sinnadurai et al. (91.4% and 90.0% following breast-conserving surgery and mastectomy, respectively) [13,25]. Lower survival rates have been reported by Khongthong et al. (66.2%) [26], possibly reflecting differences in patient populations and clinical factors. However, the limited follow-up in the present study may lead to an overestimation of long-term outcomes.
The present study has several limitations. First, the retrospective single-center design may limit the generalizability of the findings to broader populations. Second, missing data for several variables, including Ki-67, hormone receptor status, and tumor grade, reduced the sample size available for some analyses. Finally, the relatively short median follow-up of 30 months, with 11.9% of patients having less than 12 months of follow-up, limits the interpretation of survival outcomes and warrants longer follow-up to confirm the durability of the observed favorable trajectory.
Conclusion
High tumor grade in BCYW was significantly associated with TNBC, ER-negative, and PR-negative status, but not with HER2 expression. Ki-67 was significantly higher in Grade III tumors, while symptom duration showed no correlation with tumor size, reinforcing the aggressive tumor biology of BCYW.
Declarations
Conflicts of interest: The authors have no conflicts of interest to disclose.
Ethical approval: In accordance with our institution's oral policy, retrospective cohort studies involving anonymized histopathological material and de-identified patient data do not require formal ethical approval.
Patient consent (participation and publication): Informed consent was obtained from all patients for the use of their clinical data and for publication.
Funding: The present study received no financial support.
Acknowledgements: None to be declared.
Authors' contributions: SLT, AMS, and AAQ contributed to the study conception and design, were responsible for managing the cases and surgical care, and critically reviewed the manuscript. LRAP performed the radiological assessment and interpretation and critically reviewed the manuscript. AMA performed the histopathological assessment and critically reviewed the manuscript. MKA, BTM, HHF, SNA, SRQ, and VIJ collected the clinical data, conducted patient follow-up, and critically reviewed the manuscript. MTH contributed to the study conception and design, conducted the literature review, performed the data analysis, prepared the tables, and wrote the first draft of the manuscript. HOA critically reviewed the manuscript. All authors read and approved the final manuscript.
Use of AI: Claude Opus 4.7 (Anthropic) was used to assist with language review and grammar checking.
Data availability statement: The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
- Zhang W, Wu S, Liu J, Zhang X, Ma X, Yang C, et al. Metastasis patterns and prognosis in young breast cancer patients: A SEER database analysis. Frontiers in oncology. 2022;12:872862. doi:10.3389/fonc.2022.872862
- Zuhair D. Hammood, Abdulwahid M. Salih, Snur Othman, Berwn A. Abdulla, Shvan H. Mohammed, Fahmi H. Kakamad, et al. Breast cancer recurrence 27 years after full recovery; A case report with literature review. International Journal of Surgery Case Reports. 2022;92:1-3. doi:10.1016/j.ijscr.2022.106827
- McVeigh UM, Tepper JW, McVeigh TP. A review of breast cancer risk factors in adolescents and young adults. Cancers. 2021;13(21):5552. doi:10.3390/cancers13215552
- Chekhun V, Martynyuk О, Lukianova Y, Mushii O, Zadvornyi T, Lukianova N. Features of breast cancer in patients of young age: search for diagnosis optimization and personalized treatment. Experimental Oncology. 2023;45(2):139-50. doi:10.15407/exp-oncology.2023.02.139
- Sharma DK, Saripilli R. Recent strategies in diagnosis, screening, prevention, and treatment of breast cancer in young women. Discover Oncology. 2025;16(1):1532. doi:10.1007/s12672-025-03180-0
- Malekzadeh Moghani M, Hashemi AS, Bazgir N. Clinicopathological characteristics and outcome of very young breast cancer patients at a referral center in Iran. J Clin Oncol. 2023;41(16_suppl):e12568. doi:10.1200/JCO.2023.41.16_suppl.e12568
- Alhaidary AA, Al-Qudimat AR, Arabi H, Al-Zoubi RM. Imaging patterns in breast cancer for women under 40 years: a descriptive cohort study. Journal of Epidemiology and Global Health. 2024;14(1):63-71. doi:10.1007/s44197-023-00169-2
- Ahmed A, Sheikha A, Abdulla H, Ahmed K, Mula-Hussain L. Breast cancer in young women: A clinicopathological hospital-based descriptive study from Kurdistan, Iraq. Middle East Journal of Cancer. 2021;12(1):137-42. doi:10.30476/mejc.2020.82210.1068
- Den J, Nelson N, Vaghjiani R, Tyler D, Klimberg VS. Rising Breast Cancer Incidence and Poor Outcomes in Young Women: A Retrospective Study. The Breast Journal. 2026;2026(1):5584726. doi:10.1155/tbj/5584726
- Murphy BL, Day CN, Hoskin TL, Habermann EB, Boughey JC. Adolescents and Young Adults with Breast Cancer have More Aggressive Disease and Treatment Than Patients in Their Forties: BL Murphy et al. Annals of Surgical Oncology. 2019;26(12):3920-30. doi:10.1245/s10434-019-07653-9
- Muhialdeen AS, Ahmed JO, Baba HO, Abdullah IY, Hassan HA, Najar KA, et al. Kscien’s list: a new strategy to discourage predatory journals and publishers (second version). Barw Med J. 2023;1(1):24–26. doi:10.58742/bmj.v1i1.14
- Koo MM, Von Wagner C, Abel GA, McPhail S, Rubin GP, Lyratzopoulos G. Typical and atypical presenting symptoms of breast cancer and their associations with diagnostic intervals: Evidence from a national audit of cancer diagnosis. Cancer Epidemiology. 2017;48:140-6. doi:10.1016/j.canep.2017.04.010
- El Saghir NS, Khalil LE, El Dick J, Atwani RW, Safi N, Charafeddine M, et al. Improved survival of young patients with breast cancer 40 years and younger at diagnosis. JCO Global Oncology. 2023;9:e2200354. doi:10.1200/GO.22.00354
- Eugênio DS, Souza JA, Chojniak R, Bitencourt AG, Graziano L, Souza EF. Perfil do câncer de mama em mulheres com idade inferior a 40 anos. Revista da Associação Médica Brasileira. 2016;62:755-61. doi:10.1590/1806-9282.62.08.755
- Anwar SL, Raharjo CA, Herviastuti R, Dwianingsih EK, Setyoheriyanto D, Avanti WS, et al. Pathological profiles and clinical management challenges of breast cancer emerging in young women in Indonesia: a hospital-based study. BMC Women's Health. 2019;19(1):28. doi:10.1186/s12905-019-0724-3
- Sopik V, Lubiński J, Gronwald J, Huzarski T, Cybulski C, Tryggvadóttir L, et al. An international cohort study of breast cancer survival in young women. BJC reports. 2026;4(1):6. doi:10.1038/s44276-026-00207-z
- Unger-Saldaña K, Fitch-Picos K, Villarreal-Garza C. Breast cancer diagnostic delays among young Mexican women are associated with a lack of suspicion by health care providers at first presentation. Journal of Global Oncology. 2019;5:1-2. doi:10.1200/JGO.19.00093
- Costa L, Kumar R, Villarreal-Garza C, Sinha S, Saini S, Semwal J, et al. Diagnostic delays in breast cancer among young women: An emphasis on healthcare providers. The Breast. 2024;73:103623. doi:10.1016/j.breast.2023.103623
- Tzikas AK, Nemes S, Linderholm BK. A comparison between young and old patients with triple-negative breast cancer: biology, survival, and metastatic patterns. Breast Cancer Research and Treatment. 2020;182(3):643-54. doi:10.1007/s10549-020-05727-x
- Zhu JW, Charkhchi P, Adekunte S, Akbari MR. What is known about breast cancer in young women?. Cancers. 2023;15(6):1917. doi:10.3390/cancers15061917
- Ayatollahi H, Jafarian AH, Moghadam ZP, Ayatollahi Y, Hassankhani GG, Mehrad-Majd H. Clinicopathological Characteristics of Breast Cancer Patients with Equivocal Immunohistochemistry: A Prevalence-Based Statistical Analysis. Iranian Journal of Pathology. 2025 ;20(3):273. doi:10.30699/ijp.2025.2045071.3378
- Abubakr A, Humayun S, Ali T, Khursheed S, Khan A, Khan S, et al. Correlation between Ki-67 expression and tumor grade in breast cancer: a cross-sectional study. Cureus. 2024;16(12). doi:10.7759/cureus.76239
- Lee J, Kim SH, Kang BJ, Lee A, Park WC, Hwang J. Imaging characteristics of young age breast cancer (YABC) focusing on pathologic correlation and disease recurrence. Scientific Reports. 2021;11(1):20205. doi:10.1038/s41598-021-99600-6
- Abulkhair O, Omair A, Makanjuola D, Al Zaid M, Al Riyees L, Abdelhafiez N, et al. Breast cancer in young women: Is it different? A single-center retrospective cohort study. Clinical Medicine Insights: Oncology.2024;18:11795549241228235. doi:10.1177/11795549241228235
- Sinnadurai S, Kwong A, Hartman M, Tan EY, Bhoo-Pathy NT, Dahlui M, et al. Breast-conserving surgery versus mastectomy in young women with breast cancer in Asian settings. BJS open. 2019;3(1):48-55. doi:10.1002/bjs5.50111
- Khongthong P, Prateepchaiboon T, Ruangsuwan T. Overall survival and prognostic factors in young women with breast cancer: a retrospective cohort study from Southern Thailand. World J Surg Oncol. 2026;24:49. doi:10.1186/s12957-026-04349-9

This work is licensed under a Creative Commons Attribution 4.0 International License.